A Two-Stage Data Mining and Randomized Controlled Trial Approach to Evaluate the Gouteng Xiakucao Formula for Essential Hypertension Comorbid with Anxiety Disorder of Liver-Yang Hyperactivity Pattern
Abstract
Essential hypertension (EH) comorbid with anxiety disorder lacks optimal pharmacological options, and Traditional Chinese Medicine (TCM) formula construction has historically relied on classical theory rather than systematic data-driven evaluation. We addressed this gap through a two-stage workflow. Stage 1 was a retrospective data mining analysis of 114 EH-anxiety patients combining association rule, factor, and hierarchical cluster analysis of TCM prescriptions; it identified Liver-Yang Hyperactivity (LYH) as the predominant syndrome (52.63%) and Gouteng-Xiakucao as the highest-confidence herb pair (support 50.88%, confidence 94.83%), and anchored construction of the Gouteng Xiakucao Formula (GXF). Stage 2 randomized 128 patients with EH-anxiety comorbidity of LYH pattern 1:1 to valsartan plus GXF or valsartan plus oryzanol for 14 days; 118 of the 128 randomized patients (60 intervention, 58 control) completed the protocol and were analyzed per protocol. The GXF arm showed significantly greater post-treatment reductions than control in systolic blood pressure (134.03 ± 8.17 vs 137.18 ± 6.92 mmHg, P = 0.026), diastolic blood pressure (80.93 ± 3.88 vs 83.42 ± 4.31 mmHg, P = 0.001), Hamilton Anxiety Rating Scale score (11.63 ± 2.66 vs 12.76 ± 3.08, P = 0.036), Pittsburgh Sleep Quality Index (P = 0.015), and TCM syndrome score (P = 0.002); the SF-36 Physical Functioning, Social Functioning, and Mental Health subscales also improved more in the GXF arm, with no clinically meaningful adverse changes. This data-anchored, expertise-refined TCM formula derived from real-world prescription mining produced greater short-term improvements than an oryzanol-based comparator in patients with EH-anxiety comorbidity of LYH pattern, although the absolute between-group differences in HAMA score did not exceed established minimal clinically important difference thresholds and the comparator is not a guideline-recommended first-line anxiolytic, so the findings should be interpreted as a signal of efficacy requiring confirmation against standard pharmacotherapy. The two-stage workflow illustrates a feasible paradigm for systematic TCM formula development and prospective validation.
1. Introduction
Essential hypertension (EH) and anxiety disorders are among the most prevalent chronic conditions worldwide, and their comorbidity represents a substantial clinical and public health burden. Hypertension affects more than 1.4 billion adults globally, with awareness, treatment, and control rates remaining suboptimal in most populations [1]. Anxiety disorders are also common, with a reported lifetime prevalence of 7.6% in the Chinese population and an estimated 100 million affected individuals [2]. The two conditions exhibit a bidirectional relationship: chronic anxiety is an independent risk factor for the development of hypertension [3], while hypertensive patients show a higher prevalence of anxiety symptoms than the general population [4]. Comorbid patients show pronounced somatization, reduced treatment adherence, impaired functioning, and diminished quality of life [4]. Proposed shared mechanisms include hypothalamic-pituitary-adrenal (HPA) axis dysregulation, autonomic imbalance, and chronic low-grade inflammation [5-7].
Current pharmacological strategies face notable limitations. The conventional approach combines standard antihypertensive agents with anxiolytic medications. Selective serotonin reuptake inhibitors (SSRIs) are commonly recommended as first-line anxiolytic therapy because of their relatively favorable cardiovascular profile [8] but show delayed onset of action. Serotonin-norepinephrine reuptake inhibitors such as venlafaxine demonstrate efficacy but may induce blood pressure fluctuations [9]; benzodiazepines act rapidly but carry risks of dependence and cognitive impairment, restricting them to short-term adjunctive use [10]; tricyclic antidepressants are limited by anticholinergic effects and cardiotoxicity. To date, no single regimen has demonstrated optimal efficacy and tolerability for EH comorbid with anxiety disorder, and the unmet clinical need persists.
Traditional Chinese Medicine (TCM) offers a complementary therapeutic framework grounded in a holistic perspective and pattern differentiation-based individualized treatment, with potential advantages in addressing multifactorial chronic conditions through multi-component formulas [11]. However, two methodological challenges have constrained the integration of TCM-based interventions into modern evidence-based care for this comorbidity. First, TCM syndrome classification for EH-anxiety comorbidity remains heterogeneous across schools and regions, lacking a standardized empirically grounded system [12]. Second, traditional formula construction has historically relied on individual physician experience and classical theoretical frameworks rather than systematic data-driven evaluation. Recent advances in real-world data mining—association rule analysis, hierarchical clustering, and factor analysis applied to prescription records—offer an opportunity to systematically identify dominant syndrome patterns and high-confidence herb combinations [13,14], anchoring formula construction in empirical regularities rather than expert opinion alone. Yet few studies have explicitly integrated such data-driven formula construction with prospective randomized controlled trial (RCT) validation within a single coherent workflow.
The present study addresses this gap through a two-stage design. In Stage 1, we conducted a retrospective data mining analysis of 114 patients with EH comorbid with anxiety disorder to identify the predominant TCM syndrome patterns and core herb combinations characterizing real-world prescription practice. Findings from Stage 1 informed the construction of the Gouteng Xiakucao Formula (GXF), with composition anchored by association rule and factor analysis results and refined through clinical expertise. In Stage 2, we conducted a randomized controlled trial in 128 patients with EH comorbid with anxiety disorder of Liver-Yang Hyperactivity (LYH) pattern, comparing GXF plus valsartan against a commonly used primary-care reference regimen. We hypothesized that GXF combined with valsartan would produce greater short-term improvements in blood pressure and anxiety severity compared with oryzanol combined with valsartan, with secondary benefits in sleep quality and health-related quality of life and an acceptable safety profile.
2. Materials and Methods
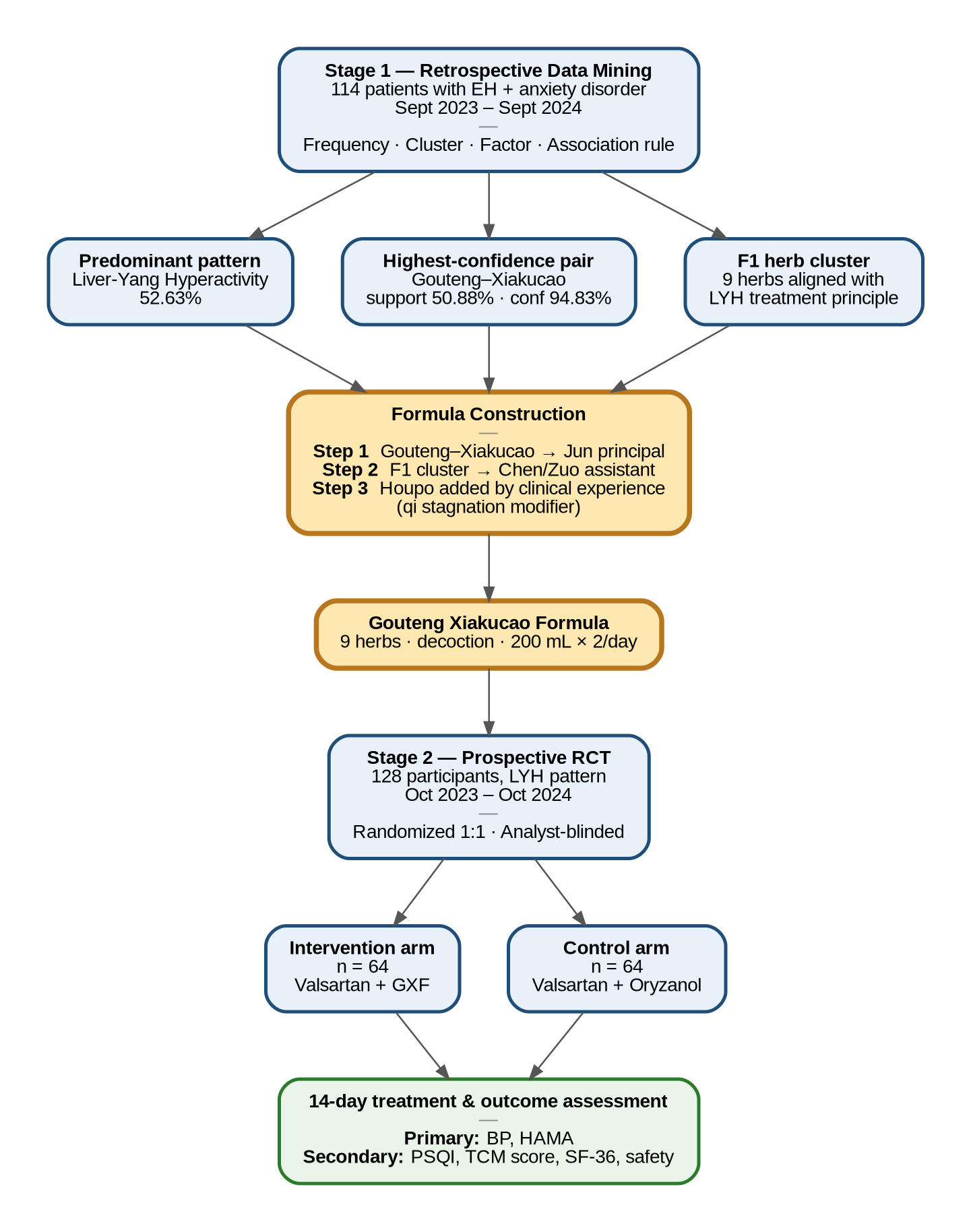
Figure 1. Study design and CONSORT participant flow.(A) Two-stage research workflow. Stage 1 (retrospective data mining of 114 patients with essential hypertension comorbid with anxiety disorder) yielded three convergent findings—predominant Liver-Yang Hyperactivity (LYH) pattern, highest-confidence herb pair Gouteng–Xiakucao, and F1 factor herb cluster—that anchored the three-step construction of the Gouteng Xiakucao Formula (GXF). Stage 2 (prospective randomized controlled trial in 128 LYH-pattern patients) compared GXF plus valsartan with oryzanol plus valsartan over 14 days. (B) CONSORT diagram of participant flow through the Stage 2 trial: 128 randomized, 10 discontinued (4 intervention, 6 control), 118 analyzed per protocol. GXF, Gouteng Xiakucao Formula; LYH, Liver-Yang Hyperactivity.
2.1. Study Design
This study employed a two-stage workflow combining retrospective data mining of real-world TCM prescriptions with a prospective randomized controlled trial. Stage 1 applied association rule analysis, factor analysis, and hierarchical clustering to medical records of patients with EH comorbid with anxiety disorder to identify dominant TCM syndrome patterns and high-confidence herb combinations. Findings from Stage 1 directly informed the construction of GXF. Stage 2 evaluated GXF in a randomized, parallel-group, single-center clinical trial in patients with the most prevalent syndrome pattern identified in Stage 1.
2.2. Stage 1: Retrospective Data Mining
Medical records of 114 patients with EH comorbid with anxiety disorder, who attended the Department of Cardiology at the Affiliated Hospital of Shandong University of Traditional Chinese Medicine between September 2023 and September 2024, were retrieved from the hospital research data platform. Inclusion criteria required (i) a confirmed diagnosis of essential hypertension and anxiety disorder based on standard biomedical and TCM criteria, (ii) complete clinical documentation, and (iii) absence of other severe comorbidities affecting prognosis. All identifiable personal information was anonymized before analysis.
Symptom, tongue, pulse, and prescription data were standardized using authoritative TCM references and the Chinese Pharmacopoeia (2020 edition) [15]. Equivalent symptom expressions were merged (e.g., "lower limb numbness" and "hand numbness" → "limb numbness"); herbs appearing in different processed forms were unified according to pharmacopoeial conventions. A binary coding scheme was applied: each symptom or herb present in a given prescription was coded as 1, absent items as 0. Data entry followed a double-entry, double-check protocol with discrepancy resolution.
Three complementary data mining techniques were applied. Frequency analysis characterized the distribution of clinical symptoms, tongue and pulse features, syndrome patterns, and herb usage. Factor analysis (principal component method, varimax rotation) was performed on high-frequency clinical features (symptoms with frequency >1%; tongue and pulse signs with frequency >5%) to identify latent syndrome elements; factors with eigenvalues >1 and loadings >0.3 were retained. Hierarchical cluster analysis (between-groups average linkage) was applied to the same feature set to identify discrete syndrome patterns, with the optimal number of clusters determined jointly by dendrogram structure and TCM clinical interpretability. The same factor and cluster analyses were applied to herbs with frequency >10% to identify core formula combinations. Association rule mining using the Apriori algorithm was performed on herbs with frequency ≥10% to identify high-confidence pairings (minimum support 10%, minimum confidence 80%, maximum antecedent size 1). SPSS Statistics 27.0 was used for factor and cluster analyses; SPSS Modeler 18.0 for association rule mining.
2.3. Formula Construction from Data Mining Findings
GXF was constructed in three steps grounded in Stage 1 results. First, the herb pair "Gouteng (Uncariae Ramulus Cum Uncis)-Xiakucao (Prunellae Spica)" was identified by association rule mining as the highest-confidence pairing (support 50.88%, confidence 94.83%) and was designated as the principal (Jun) component, directly addressing the predominant LYH pattern. Second, the F1 herb factor combination from Stage 1 factor analysis—comprising Gouteng, Tianma (Gastrodiae Rhizoma), Xiakucao, Zhizi (Gardeniae Fructus), Hehuanpi (Albiziae Cortex), Zhenzhumu (Concha Margaritiferae), Chuanniuxi (Cyathulae Radix), Chongweizi (Leonuri Fructus), and Chaohuaihua (Sophorae Flos Praeparatus)—provided the data-driven candidate set for assistant (Chen/Zuo) components. Third, candidates were refined according to the LYH treatment principle (calming the liver, suppressing yang, soothing depression, and tranquilizing the mind), with the addition of Houpo (Magnoliae Officinalis Cortex) by the senior author on the basis of clinical experience to address concomitant qi stagnation. The final formula integrates empirically high-confidence components with classical compositional principles. Because Houpo was added on the basis of clinical expertise rather than emerging directly from the association rule or factor analysis output, we describe the construction paradigm as "data-anchored, expertise-refined" rather than purely data-driven. We emphasize that this construction process was hypothesis-generating; GXF's clinical efficacy was evaluated independently in Stage 2.
2.4. Stage 2: Trial Design and Participants
Stage 2 was a randomized, parallel-group, single-center clinical trial conducted at the Affiliated Hospital of Shandong University of Traditional Chinese Medicine between October 2023 and October 2024. Eligible participants were adults aged 18-75 years with grade 1 essential hypertension diagnosed per current international and national guidelines [1]; mild-to-moderate generalized anxiety disorder diagnosed per the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) [16] with a baseline HAMA total score of 14-28; and concurrent LYH pattern based on standardized TCM syndrome differentiation methodology [17,18]. The TCM pattern diagnosis required at least one principal symptom (dizziness or headache), at least three secondary symptoms (e.g., facial flushing, irritability, dry mouth, bitter taste, limb numbness, tinnitus, dark urine, constipation), and characteristic tongue and pulse findings (red tongue with yellow coating, wiry rapid pulse), judged independently by two attending physicians or above. Exclusion criteria included secondary hypertension, grade 2 or 3 hypertension, severe organ dysfunction, severe comorbid psychiatric disorders, pregnancy or lactation, and concurrent participation in other trials.
2.5. Interventions
All participants received standardized lifestyle counseling (dietary modification, smoking cessation, alcohol moderation, weight control, regular physical activity, psychological adjustment). The control group received valsartan capsules (80 mg orally once daily, up-titrated to 160 mg if blood pressure remained uncontrolled) plus oryzanol tablets (10 mg orally three times daily). Oryzanol was selected as the comparator anxiolytic because it is widely used in Chinese primary-care settings for autonomic dysregulation and stress-related anxiety and represents the conventional non-prescription pharmacologic option in this context, although its evidence base is limited compared with first-line agents such as SSRIs (see Discussion). The intervention group received valsartan at the same dosing schedule plus GXF (Gouteng 12 g, Xiakucao 15 g, Chuanniuxi 10 g, Chongweizi 10 g, Hehuanpi 12 g, Houpo 10 g, Jiaozhizi 9 g, Chaohuaihua 10 g, Zhenzhumu 25 g), administered as a decoction in two divided doses (200 mL each) per day. All herbs were sourced from the hospital pharmacy and complied with the Chinese Pharmacopoeia (2020 edition) [15]. Both arms received treatment for 14 days.
2.6. Outcome Measures
Primary outcomes were post-treatment systolic and diastolic blood pressure and post-treatment HAMA total score. Blood pressure was measured using a calibrated automatic upper-arm sphygmomanometer following a standardized protocol (5-minute seated rest, duplicate readings 30-60 seconds apart with a third reading if the first two differed by >10 mmHg, mean of two or three readings recorded). The HAMA is a 14-item clinician-rated instrument (total score 0-56) with established validity for anxiety severity [19]. Secondary outcomes included the Pittsburgh Sleep Quality Index (PSQI; 0-21, higher scores indicating poorer sleep) [20], the standardized TCM syndrome score [17], the 36-Item Short Form Health Survey (SF-36; eight subscales each scored 0-100) [21], and ordinal clinical efficacy classifications for blood pressure, anxiety, and TCM syndrome score, defined a priori per established TCM clinical research methodology [17]. Safety outcomes comprised pre- and post-treatment complete blood count, urinalysis, stool examination, hepatic and renal function tests, electrocardiogram, and adverse event reports.
2.7. Sample Size, Randomization, and Blinding
Sample size was estimated using PASS 11 software, based on previously reported antihypertensive efficacy rates of approximately 85% in TCM-plus-antihypertensive combination arms and 77% in antihypertensive-only or weaker-comparator arms across systematic reviews and meta-analyses of TCM-based treatment for hypertension, including the Tianma Gouteng Yin formula closely related in composition to GXF [22-24]. With 80% power and a two-sided α of 0.05, 58 participants per arm were required; this was inflated to 64 per arm to accommodate an anticipated 10% attrition rate, yielding a total enrollment of 128. Randomization used a computer-generated random number sequence with a 1:1 allocation ratio (simple randomization). Allocation was concealed via sequentially numbered, opaque, sealed envelopes opened only at enrollment. Owing to the obvious sensory differences between an herbal decoction and oral tablets, neither participants nor treating clinicians could be blinded to group assignment; the statistical analyst remained blinded throughout data analysis. This study therefore employed an analyst-blinded (single-blind) design, acknowledged as a methodological limitation.
2.8. Statistical Analysis
All analyses were conducted using SPSS Statistics 27.0.1. Continuous variables were tested for normality with the Shapiro-Wilk test separately in each arm and, for within-group changes, on the paired difference scores in each arm. Normally distributed data were summarized as mean ± standard deviation and compared using independent-samples t-tests between groups and paired t-tests for within-group changes. Non-normally distributed data were summarized as median (interquartile range) and compared using the Mann-Whitney U test and Wilcoxon signed-rank test, respectively. Where the within-arm change-score distribution differed in normality between the two arms (e.g., HAMA change scores satisfied normality in the control arm but not in the intervention arm), the parametric or non-parametric within-group test appropriate to each arm was applied; this is the source of the test asymmetry observed for HAMA in Section 3.4. Categorical variables were compared using the χ² test, with continuity correction applied when expected cell counts were between 1 and 5. Ordinal efficacy classifications were compared using non-parametric rank-sum tests. Two-sided P < 0.05 was considered statistically significant. Analyses were conducted on the per-protocol population of 118 participants who completed the full study protocol (60 intervention, 58 control); a formal intent-to-treat analysis was not performed, and this is acknowledged as a methodological limitation. No interim analyses were planned and no subgroup analyses were performed.
2.9. Ethics and Trial Registration
The study was approved by the Institutional Ethics Committee of the Affiliated Hospital of Shandong University of Traditional Chinese Medicine (approval No. (2025) Lun Shen Di (006) Hao-KY, dated 16 January 2025) and conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines. Written informed consent was obtained from all participants. The trial was not prospectively registered in a public clinical-trial registry; the absence of prospective registration is acknowledged as a methodological limitation in the Discussion.
3. Results
3.1. Syndrome Distribution and Prescription Patterns
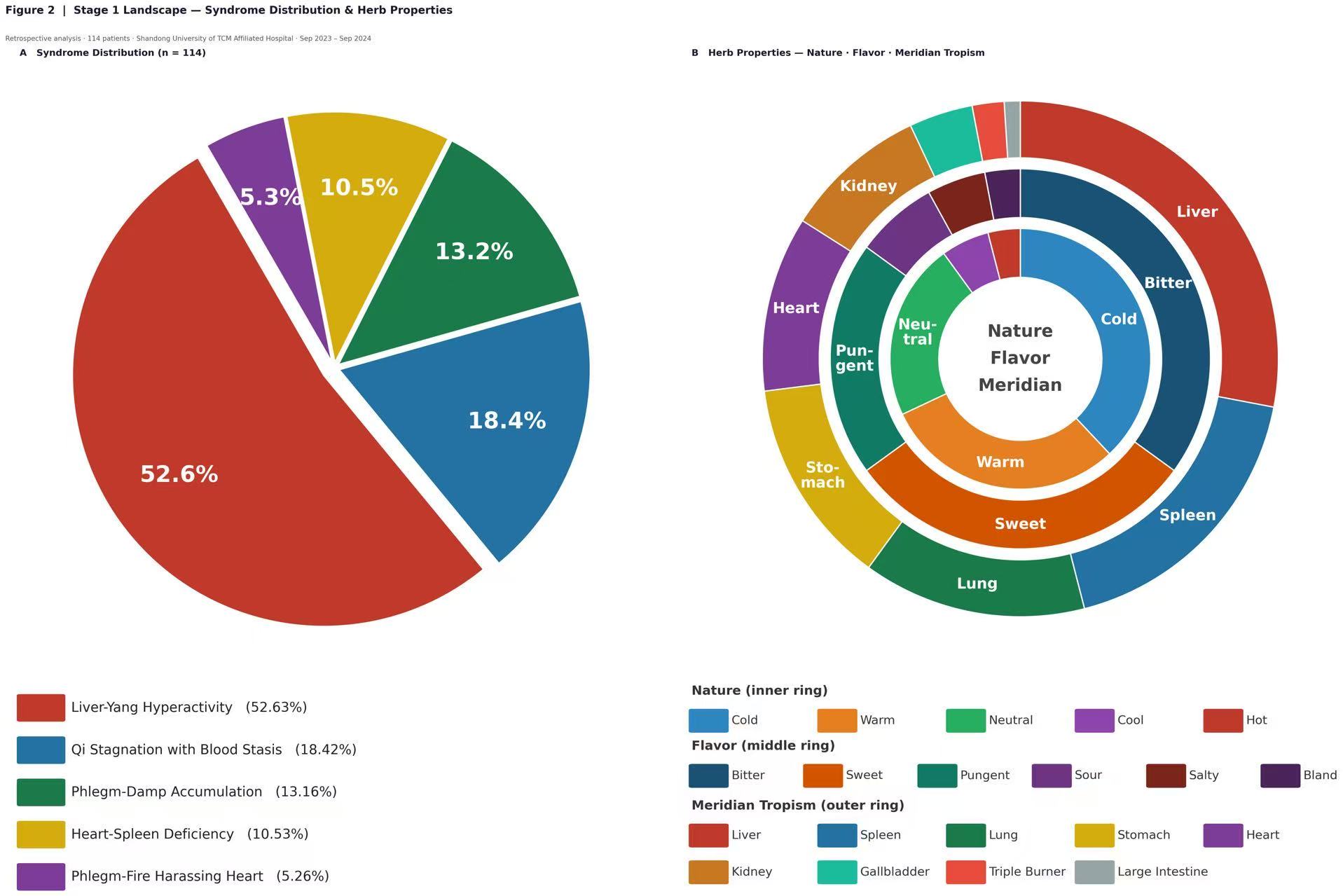
Figure 2. Stage 1 — Syndrome distribution and herb properties (n = 114). (A) Frequency distribution of five TCM syndrome patterns identified in 114 patients with EH comorbid with anxiety disorder: Liver-Yang Hyperactivity (52.63%), qi stagnation with blood stasis (18.42%), phlegm-damp accumulation (13.16%), heart-spleen deficiency (10.53%), and phlegm-fire harassing the heart (5.26%). (B) Concentric ring chart showing the distribution of herb properties across all prescriptions: nature (inner ring; cold, warm, neutral, cool, hot), flavor (middle ring; bitter, sweet, pungent, sour, salty, bland), and meridian tropism (outer ring; liver, spleen, lung, stomach, heart, kidney, gallbladder, triple burner, large intestine). EH, essential hypertension; TCM, Traditional Chinese Medicine.
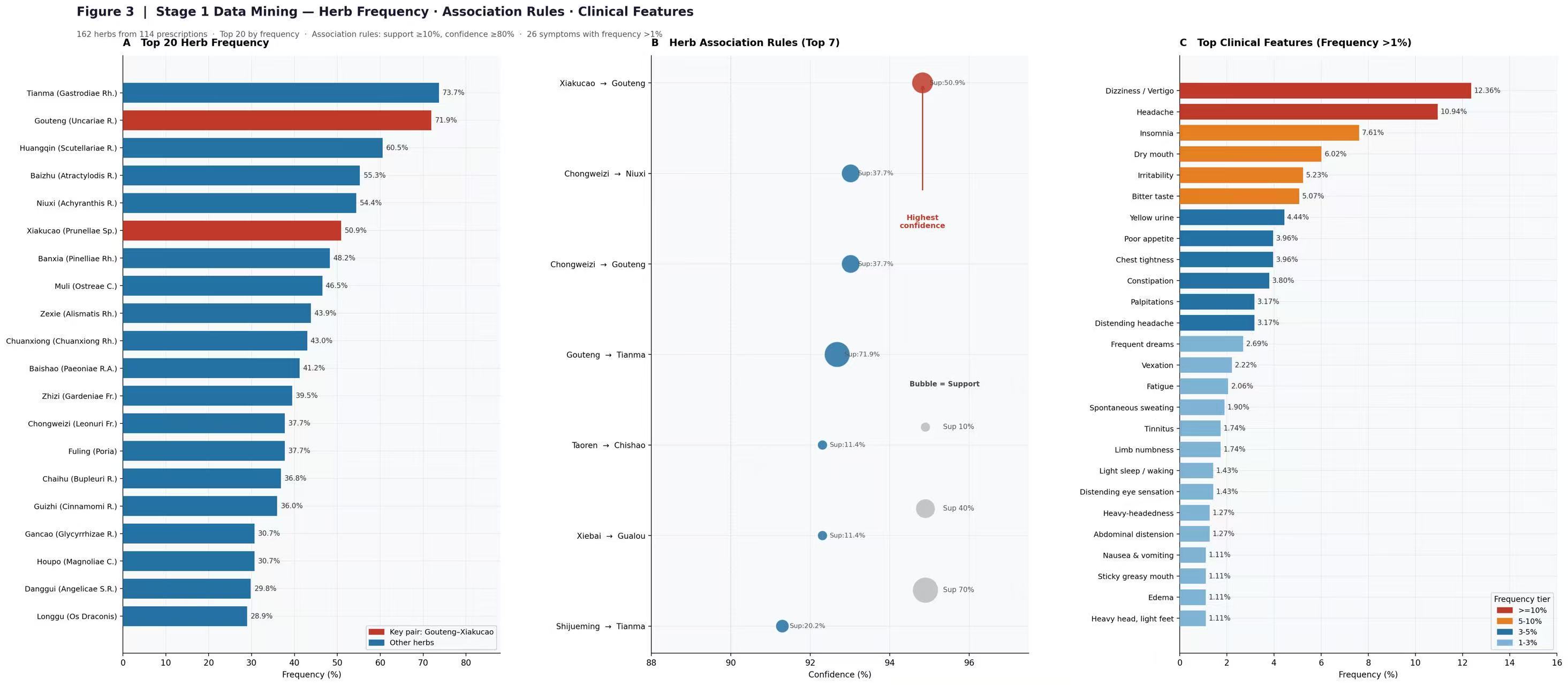
Figure 3. Stage 1 — Herb frequency, association rules, and clinical features (n = 114). (A) Top 20 most frequently prescribed herbs across 162 distinct herbs used in 114 prescriptions; the Gouteng–Xiakucao key pair is highlighted in red. (B) Association rules identified by the Apriori algorithm with herbs as both antecedents and consequents (minimum support 10%, minimum confidence 80%, maximum antecedent size 1); the top 7 rules ranked by confidence are displayed. Bubble size represents support and the x-axis represents confidence. The Xiakucao → Gouteng rule (support 50.9%, confidence 94.83%; highlighted in red) is the highest-confidence pairing in the dataset and was designated as the principal (Jun) component of GXF. (C) Top clinical features (symptoms, tongue and pulse signs) with frequency >1%, color-coded by frequency tier (red ≥10%, orange 5–10%, blue 3–5%, light blue 1–3%). GXF, Gouteng Xiakucao Formula.
Among the 114 retrospectively analyzed patients, frequency analysis identified five TCM syndrome patterns: LYH (60/114, 52.63%), qi stagnation with blood stasis (21/114, 18.42%), phlegm-damp accumulation (15/114, 13.16%), heart-spleen deficiency (12/114, 10.53%), and phlegm-fire harassing the heart (6/114, 5.26%) (Figure 2A). The most frequent symptoms were dizziness (12.36%), headache (10.94%), insomnia (7.61%), dry mouth (6.02%), and irritability (5.23%); a wiry pulse predominated (45.45%), and the most common tongue findings were a red tongue body (27.03%) with a yellow coating (19.31%). The full distribution of high-frequency clinical features is shown in Figure 3C. Across the 114 prescriptions, 162 distinct herbs were used over 2,227 total occurrences; herb properties were predominantly cold, warm, or neutral in nature; bitter, sweet, or pungent in flavor; and tropic to the liver, spleen, lung, stomach, and heart meridians (Figure 2B).
3.2. Core Herb Pair and Formula Factor Structure
The top 20 most commonly prescribed herbs are shown in Figure 3A, led by Tianma (73.68%), Gouteng (71.93%), Huangqin (60.53%), Baizhu (55.26%), Niuxi (54.39%), and Xiakucao (50.88%). Apriori association rule mining identified the herb pair Gouteng-Xiakucao as the highest-confidence pairing (support 50.88%, confidence 94.83%), followed by Chuanniuxi-Chongweizi (37.72%, 93.02%), Gouteng-Chongweizi (37.72%, 93.02%), Tianma-Gouteng (71.93%, 92.68%), and Tianma-Shijueming (20.18%, 91.30%) (Figure 3B). Hierarchical cluster analysis of 57 herbs with prescription frequency >10% identified eight herb clusters; the first cluster encompassed herbs most aligned with the LYH treatment principle, including Tianma, Gouteng, Xiakucao, Zhizi, Hehuanpi, Zhenzhumu, Chuanniuxi, Chongweizi, and others. Factor analysis of the same 57 herbs (KMO = 0.530; Bartlett's χ² = 2616.8, P < 0.001; cumulative variance 71.04%) yielded eight interpretable factor combinations corresponding to classical formula structures. Factor 1 (F1) loaded most strongly on Gouteng (0.804), Tianma (0.782), Hehuanpi (0.789), Yimucao (0.737), Shouwuteng (0.691), Nüzhenzi (0.686), Duzhong (0.661), Zhenzhumu (0.631), Zhizi (0.608), and additional liver-yang-regulating herbs, mapping closely onto the classical Tianma Gouteng Decoction structure. This F1 combination provided the data-derived candidate set used in formula construction (Methods 2.3).
3.3. Baseline Characteristics
Of the 128 participants enrolled in Stage 2, 118 completed the protocol (60 intervention, 58 control); 10 participants withdrew (4 intervention, 6 control) due to poor adherence, protocol violation, or voluntary withdrawal (Figure 1B). The two arms were comparable at baseline in age, sex distribution, BMI, smoking and drinking history, prevalence of diabetes, coronary artery disease, prior cerebral infarction, and disease duration (all P > 0.05; Table 1).
Table 1. Baseline characteristics of participants in Stage 2.
| Variable | Category | Control (n=58) | Intervention (n=60) | Statistic | P value |
|---|---|---|---|---|---|
| Age (years) | 48.19 ± 11.89 | 46.90 ± 10.78 | t = -0.618 | 0.538 | |
| Sex (M/F) | 31/27 | 31/29 | χ² = 0.038 | 0.846 | |
| BMI (kg/m²) | 24.51 (23.12, 26.63) | 25.00 (23.54, 27.67) | Z = -1.464 | 0.143 | |
| Smoking | No / Yes | 36 / 22 | 38 / 22 | χ² = 0.020 | 0.887 |
| Drinking | No / Yes | 31 / 27 | 35 / 25 | χ² = 0.286 | 0.539 |
| Diabetes | No / Yes | 49 / 9 | 53 / 7 | χ² = 0.373 | 0.541 |
| Coronary disease | No / Yes | 52 / 6 | 56 / 4 | χ² = 0.149 | 0.699 |
| Cerebral infarction | No / Yes | 55 / 3 | 59 / 1 | χ² = 0.295 | 0.587 |
| Disease duration (years) | 3 (1, 8.25) | 4 (1, 6) | Z = -0.246 | 0.805 |
Continuous variables: mean ± SD or median (IQR). Categorical variables: counts. Statistical tests: t-test, Mann-Whitney U, χ² as appropriate.
3.4. Primary Outcomes
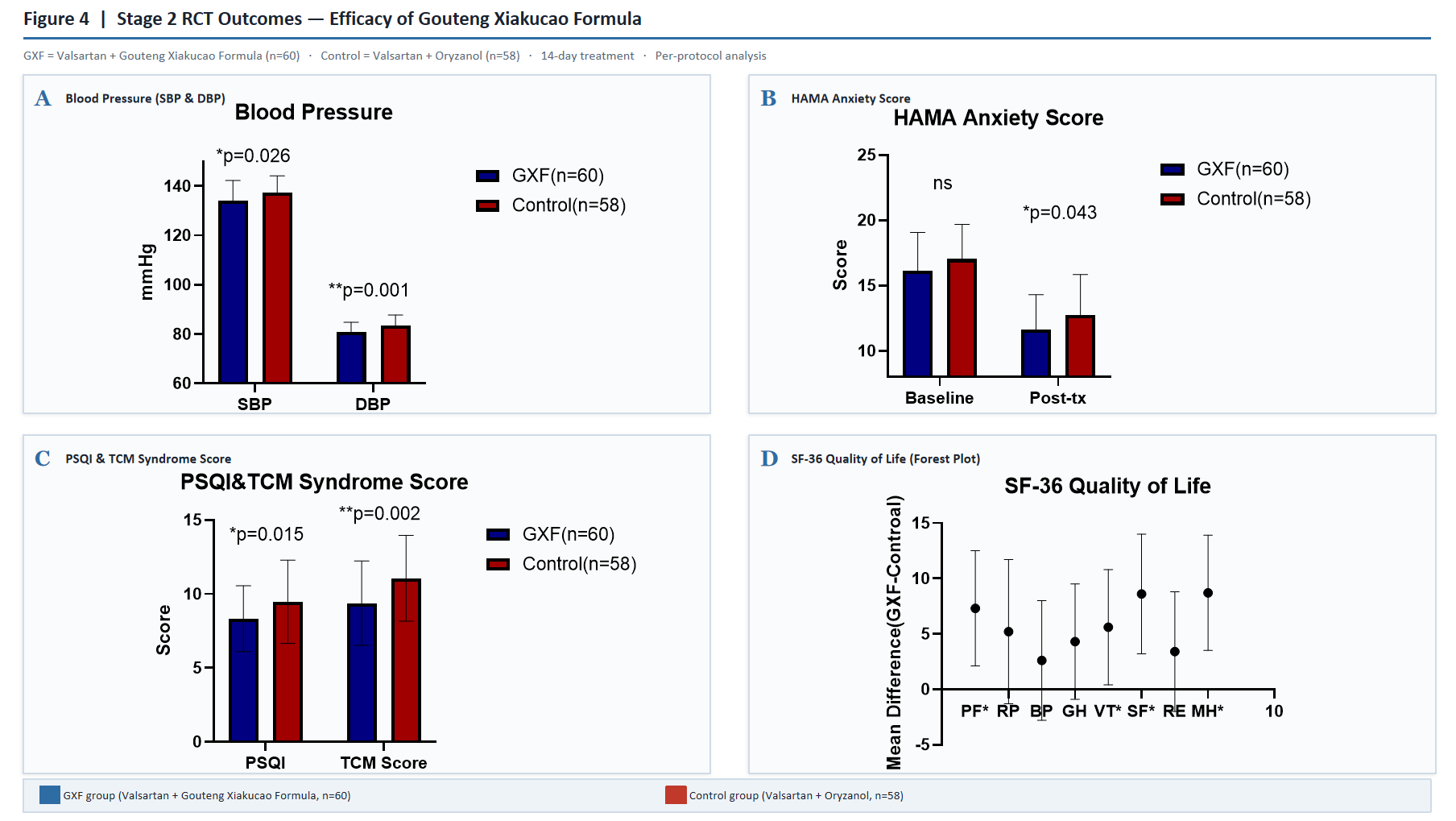
Figure 4. Stage 2 — Outcomes of the Gouteng Xiakucao Formula trial (per-protocol analysis; n = 60 intervention, n = 58 control). (A) Systolic and diastolic blood pressure (mmHg) at baseline and after 14 days of treatment in the GXF (Valsartan + GXF) and control (Valsartan + Oryzanol) arms. (B) Hamilton Anxiety Rating Scale (HAMA) total score at baseline and after 14 days. (C) Pittsburgh Sleep Quality Index (PSQI) and TCM syndrome score at post-treatment. (D) Forest plot of mean differences (GXF - Control) for the eight SF-36 subscales; significant subscales (P < 0.05) are marked with an asterisk: Physical Functioning (PF), Social Functioning (SF), and Mental Health (MH). RP, Role-Physical; BP, Bodily Pain; GH, General Health; VT, Vitality; RE, Role-Emotional. Data are mean ± SD for normally distributed variables and median (IQR) for non-normally distributed variables. Statistical tests: independent-samples t-test, Mann-Whitney U test, paired t-test, or Wilcoxon signed-rank test as appropriate. *P < 0.05, **P < 0.01. ns, not significant.
Blood pressure. Both arms showed significant within-group reductions in systolic and diastolic blood pressure after 14 days of treatment (all P < 0.001). Between-group comparisons favored the intervention arm: post-treatment systolic blood pressure was 134.03 ± 8.17 mmHg versus 137.18 ± 6.92 mmHg in the control group (t = 2.255, P = 0.026), and post-treatment diastolic blood pressure was 80.93 ± 3.88 mmHg versus 83.42 ± 4.31 mmHg (t = 3.301, P = 0.001) (Figure 4A). Categorical antihypertensive efficacy was higher in the intervention arm (19 markedly improved, 30 improved, 11 unchanged; total 81.67%) than in the control arm (10 markedly improved, 25 improved, 23 unchanged; 60.34%) (P = 0.008).
Anxiety severity. HAMA total scores decreased significantly within both arms (intervention: 16.12 ± 2.95 to 11.63 ± 2.66, Z = -6.602, P < 0.001; control: 17.03 ± 2.65 to 12.76 ± 3.08, t = 17.670, P < 0.001). Post-treatment HAMA was lower in the intervention arm (11.63 ± 2.66 vs 12.76 ± 3.08, t = -2.126, P = 0.036) (Figure 4B). Categorical anti-anxiety efficacy was higher in the intervention arm (3 cured, 7 markedly improved, 35 improved, 15 unchanged; total 75.0%) than in the control arm (1 cured, 3 markedly improved, 31 improved, 23 unchanged; 60.34%) (P = 0.039).
3.5. Secondary Outcomes
Sleep quality and TCM syndrome score. PSQI total scores decreased in both arms (intervention: 11.45 ± 3.89 to 8.33 ± 2.22; control: 11.07 ± 4.07 to 9.48 ± 2.81; both within-group P < 0.001). Post-treatment PSQI was lower in the intervention arm (8.33 ± 2.22 vs 9.48 ± 2.81, t = 2.465, P = 0.015). TCM syndrome scores also decreased in both arms (intervention: 18.13 ± 3.21 to 9.38 ± 2.85; control: 18.79 ± 3.42 to 11.07 ± 2.90; both P < 0.001) with greater post-treatment reduction in the intervention arm (9.38 ± 2.85 vs 11.07 ± 2.90, t = 2.255, P = 0.002). Categorical TCM efficacy was higher in the intervention arm (80.0% vs 65.52%, P = 0.036) (Figure 4C).
Health-related quality of life. Within-group improvements were observed in both arms across multiple SF-36 subscales (P < 0.05). Between-group comparisons identified significantly greater post-treatment improvements in the intervention arm in three subscales: Physical Functioning (median [IQR] 85.00 [80.00, 95.00] vs 85.00 [78.78, 90.00], Z = -2.016, P = 0.044), Social Functioning (75.00 [62.50, 87.50] vs 62.50 [50.00, 75.00], Z = -2.046, P = 0.041), and Mental Health (77.00 ± 7.85 vs 74.07 ± 7.61, t = -2.058, P = 0.042). The remaining five subscales (Role-Physical, Bodily Pain, Vitality, Role-Emotional, General Health) showed no significant between-group differences (Figure 4D).
3.6. Safety
Adverse events were captured by spontaneous participant report at scheduled follow-up visits and through pre- and post-treatment safety laboratory panels. No clinically significant changes were observed in any pre- or post-treatment safety parameter (complete blood count, urinalysis, stool examination, hepatic and renal function, electrocardiogram) in either arm. No adverse events related to study interventions were reported during the 14-day treatment period.
4. Discussion
This study presents a two-stage research workflow integrating retrospective real-world data mining with a prospective randomized controlled trial for the development and evaluation of a TCM intervention targeting EH comorbid with anxiety disorder. Stage 1 identified LYH as the predominant TCM syndrome pattern (52.63%) and the Gouteng-Xiakucao herb pair as the highest-confidence component combination (94.83%) in real-world prescriptions. Building on these findings, GXF was constructed and evaluated in Stage 2, where it produced significantly greater reductions than the oryzanol-based comparator in blood pressure, HAMA score, PSQI score, and TCM syndrome score, along with selective improvements in SF-36 Physical Functioning, Social Functioning, and Mental Health subscales, while maintaining a favorable short-term safety profile.
A data-anchored, expertise-refined approach to TCM formula construction. A central methodological feature of this study is the explicit linkage between empirical prescription patterns and formula construction. Traditional approaches to TCM formula design rely on classical theoretical frameworks and individual physician experience, introducing variability and limiting generalizability across practice settings. Recent applications of data mining to large prescription datasets have shown that association rule analysis and factor analysis can identify reproducible herb combinations and disease-specific compositional patterns [13]. Network pharmacology studies further indicate that such empirically derived combinations engage coherent biological target networks, including pathways involved in vascular regulation, oxidative stress, and inflammation [14]. By anchoring GXF's principal component on the highest-confidence herb pair from data mining, selecting assistant components from the corresponding factor analysis cluster, and refining the final composition with senior clinical input (notably the addition of Houpo for concomitant qi stagnation), this study illustrates a reproducible workflow for translating real-world prescription regularities, complemented by expert judgement, into a testable formula. The resulting formula was treated as a hypothesis to be tested in Stage 2 rather than as an established therapy—a distinction essential for methodological rigor in TCM clinical research.
Pharmacological basis of the formula components. The observed clinical effects of GXF are consistent with the pharmacological profiles of its principal constituents. The indole alkaloids rhynchophylline and isorhynchophylline from Uncaria rhynchophylla exert vasorelaxant effects largely independent of endothelial integrity, primarily through inhibition of L-type voltage-gated calcium channels in vascular smooth muscle [25,26]. Ethanolic extracts of U. rhynchophylla additionally engage nitric oxide-cyclic guanosine monophosphate signaling and modulate G protein-coupled receptor pathways, supporting multi-mechanism vasodilation [14]. Prunella vulgaris extracts inhibit vascular smooth muscle cell proliferation and reduce vascular inflammation through ERK/p38 MAPK and NF-κB pathway suppression [27]. Magnolol and honokiol from Magnolia officinalis are positive allosteric modulators of synaptic and extrasynaptic GABA-A receptors [28], with additional anxiolytic activity attributed to CB1 receptor modulation in honokiol-enriched preparations [29]. Albizia julibrissin contains lignan glycosides that noncompetitively inhibit the serotonin transporter and modulate the HPA axis [30,31]; geniposide from Gardenia jasminoides produces antidepressant- and anxiolytic-like effects in chronic stress models through HPA axis regulation, neuroinflammation suppression, and PI3K/Akt/GSK3β signaling [32,33].
Three convergent therapeutic axes can be hypothesized across GXF's constituent herbs that map onto the shared pathophysiology of hypertension-anxiety comorbidity, based on the preclinical literature cited above. We emphasize that these are mechanistic hypotheses extrapolated from in vitro and animal-model studies of individual constituents; the present trial did not measure CB1 receptor occupancy, PI3K/Akt/GSK3β pathway activity, IL-6/IL-17 inflammatory markers, or any other molecular endpoint, and these axes therefore await direct biomarker-level verification in future mechanistic work. (i) Direct vascular regulation via Uncaria alkaloids (L-type calcium channel blockade) and Prunella extracts (MAPK/NF-κB suppression of smooth muscle proliferation and inflammation). (ii) Central anxiolytic and stress-axis modulation via Magnolia (GABA-A potentiation and CB1 modulation), Albizia (serotonin transporter inhibition), and Gardenia (HPA-axis normalization through PI3K/Akt/GSK3β signaling). (iii) Shared regulation of comorbidity pathways via constituents acting on inflammation (IL-6, IL-17), oxidative stress (reactive oxygen species accumulation), and autonomic balance in both vascular and neural tissues. This multi-target convergence offers a plausible, but not yet empirically validated, mechanistic framework for the dual cardiovascular and anxiolytic effects observed in Stage 2 and aligns with the multi-component, multi-target paradigm increasingly recognized as a defining strength of TCM formulations.
Mechanistic convergence between hypertension and anxiety. The simultaneous improvement in blood pressure and HAMA score in the intervention arm aligns with current understanding of the shared pathophysiology of hypertension-anxiety comorbidity. A recent comprehensive review identified HPA axis hyperactivity, sympathetic nervous system imbalance, IL-6- and IL-17-mediated inflammation, and reactive oxygen species accumulation as core mechanisms linking the two conditions [4]. Whether the observed clinical benefits reflect direct cardiovascular pharmacology, indirect downstream effects of anxiety reduction, or coordinated multi-target action cannot be disentangled from the present data; this question warrants investigation through future studies incorporating biomarkers of HPA activation, sympathetic tone, and systemic inflammation.
Limitations. Several limitations should be acknowledged. First, the trial was conducted at a single center, limiting generalizability to populations with different demographic and prescribing characteristics. Second, the 14-day treatment duration was selected to capture the relief of acute hypertensive and anxiety symptoms in the LYH pattern, consistent with the conventional short-term observation window for symptom-targeted ("biaozheng") phases in TCM clinical research; it was sufficient to assess short-term efficacy and safety but cannot inform conclusions regarding sustained benefit, post-treatment relapse, or long-term tolerability. Third, owing to the obvious sensory differences between an herbal decoction and oral tablets, neither participants nor treating clinicians could be blinded; only the data analyst was blinded. Because the HAMA, PSQI, TCM syndrome score, and SF-36 subscales rely substantially on participant self-report or assessor judgment, the absence of participant and assessor blinding may have inflated the apparent between-group differences on these subjective endpoints through performance and detection bias; the use of standardized, validated scoring instruments mitigates but does not eliminate this risk, and the convergence of the subjective endpoints with the objective blood pressure result provides only partial reassurance. Fourth, the comparator regimen included oryzanol rather than a first-line anxiolytic such as an SSRI or an attention-control placebo. While this reflects common primary-care practice in the relevant clinical setting, oryzanol is not a guideline-recommended anxiolytic and is a relatively weak comparator, so the between-group differences observed here should be interpreted as evidence of activity rather than as evidence of equivalence or superiority to evidence-based pharmacotherapy [8]. Importantly, although the between-group difference in post-treatment HAMA score was statistically significant, the absolute magnitude (approximately 1.13 points on the 0-56 HAMA scale) is below the commonly cited minimal clinically important difference threshold of 3-4 points; the result should therefore be regarded as a statistically detectable signal rather than as a substantial clinical improvement perceptible to individual patients. Fifth, analyses were conducted on the per-protocol population (118 of 128 randomized participants) without a formal intent-to-treat analysis; because the four intervention-arm and six control-arm discontinuations were excluded, the per-protocol estimates may overstate efficacy if non-completion was non-random with respect to outcome. Future trials should adopt intention-to-treat as the primary analytic framework and follow modern reporting standards including the CONSORT extension for Chinese Herbal Medicine Formulas [34]. Finally, blood pressure measurements were limited to office readings; ambulatory blood pressure monitoring would have provided a more robust assessment. We also note that the trial was not prospectively registered in a public clinical-trial registry; while this does not affect the conduct or analysis of the study, prospective registration is now recommended best practice and will be implemented in future trials of this formula.
Future directions. Multi-center trials with larger and more diverse samples would strengthen external validity. Comparator arms incorporating SSRIs or attention-matched placebos would clarify the relative efficacy of GXF against current evidence-based standards. Longer follow-up with ambulatory blood pressure monitoring would address durability of effect. Mechanistic substudies measuring HPA axis activation (cortisol, ACTH), sympathetic activity (heart rate variability, plasma catecholamines), and inflammatory markers (IL-6, hs-CRP) could elucidate the specific pathways through which the formula exerts its dual cardiovascular and anxiolytic effects. The data-anchored, expertise-refined formula construction paradigm illustrated here may also be applied to other prevalent comorbidity patterns in TCM clinical practice, providing a framework for systematically translating empirical prescription regularities into testable interventions.
5. Conclusions
GXF, a data-anchored, expertise-refined TCM formula constructed by integrating association rule and factor analysis findings from real-world prescriptions with senior clinical input, produced statistically greater short-term improvements than an oryzanol-based comparator in blood pressure, anxiety severity, sleep quality, TCM syndrome score, and selected health-related quality-of-life domains in patients with EH comorbid with anxiety disorder of LYH pattern, with an acceptable 14-day safety profile. The absolute between-group difference on the HAMA scale did not exceed conventional minimal clinically important difference thresholds, and the comparator was not a first-line anxiolytic, so the findings should be regarded as a signal of efficacy requiring confirmation rather than as evidence of clinical superiority over standard pharmacotherapy. These findings nevertheless support the feasibility of a two-stage research workflow combining retrospective data mining with prospective randomized controlled validation as a paradigm for systematic TCM formula development. Larger, longer, multi-center, intention-to-treat, and active-comparator-controlled trials are warranted to confirm efficacy, establish durability, and elucidate mechanisms.
Author Contributions
Conceptualization, Y.W.; methodology, Y.W. and X.W.; data curation, X.W. and X.S.; formal analysis, X.W. and X.S.; investigation, X.W. and X.S.; writing—original draft preparation, X.W.; writing—review and editing, Y.W., X.W., and X.S.; supervision, Y.W.; project administration, Y.W. All authors have read and agreed to the published version of the manuscript. # These authors contributed equally to this work.
Funding
This study was supported by the 2023 Jinan Clinical Medical Science and Technology Innovation Plan (No. 202328087); the Medical and Health Science and Technology Development Project of Shandong Province (No. 202003011161); and the 2025 National Integrated Reform Demonstration Zone for Traditional Chinese Medicine Science and Technology Joint Construction Project: Integration and Mechanism Exploration of Diagnosis and Treatment Protocol for Sepsis Based on the Lu School’s Theory of “Qi Mechanism Reversal” in Acute Conditions.
Informed Consent Statement
Written informed consent was obtained from all participants prior to enrollment.
Data Availability Statement
The de-identified datasets generated and analyzed during the current study, and the trial protocol, are available from the corresponding author upon reasonable request, subject to institutional and ethical approval.
Acknowledgments
The authors thank the staff of the Department of Cardiology and the Pharmacy Department of the Affiliated Hospital of Shandong University of Traditional Chinese Medicine for their support of this study.
Conflicts of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
-
T. Unger, C. Borghi, F. Charchar, N. A. Khan, N. R. Poulter, D. Prabhakaran, A. Ramirez, M. Schlaich, G. S. Stergiou, M. Tomaszewski, R. D. Wainford, B. Williams, A. E. Schutte. “2020 international society of hypertension global hypertension practice guidelines.” Hypertension 2020, 75, 6, 1334-57.
-
Y. Huang, Y. Wang, H. Wang, Z. Liu, X. Yu, J. Yan, Y. Yu, C. Kou, X. Xu, J. Lu, Z. Wang, S. He, Y. Xu, Y. He, T. Li, W. Guo, H. Tian, G. Xu, X. Xu, Y. Ma, L. Wang, L. Wang, Y. Yan, B. Wang, S. Xiao, L. Zhou, L. Li, L. Tan, T. Zhang, C. Ma, Q. Li, H. Ding, H. Geng, F. Jia, J. Shi, S. Wang, N. Zhang, X. Du, X. Du, Y. Wu. “Prevalence of mental disorders in China: a cross-sectional epidemiological study.” Lancet, Psychiatry 2019, 6, 3, 211-24.
-
L.-F. Lim, M. Solmi, S. Cortese. “Association between anxiety and hypertension in adults: a systematic review and meta-analysis.” Neurosci. Biobehav. Rev. 2021, 131, 96-119.
-
T. Qiu, Z. Jiang, X. Chen, Y. Dai, H. Zhao. “Comorbidity of anxiety and hypertension: common risk factors and potential mechanisms.” Int. J. Hypertens. 2023, 2023, 9619388.
-
J. M. Saavedra, E. Sánchez-Lemus, J. Benicky. “Blockade of brain angiotensin II AT1 receptors ameliorates stress, anxiety, brain inflammation and ischemia: therapeutic implications.” Psychoneuroendocrinology 2011, 36, 1, 1-18.
-
D. Hering, K. Lachowska, M. Schlaich. “Role of the sympathetic nervous system in stress-mediated cardiovascular disease.” Curr. Hypertens. Rep. 2015, 17, 10, 80.
-
L. Xiao, D. G. Harrison. “Inflammation in hypertension.” Can. J. Cardiol 2020, 36, 5, 635-47.
-
M. E. Thase, K. G. Larsen, E. Reines, S. H. Kennedy. “The cardiovascular safety profile of escitalopram.” Eur. Neuropsychopharmacol.: J. Eur. Coll. Neuropsychopharmacol. 2013, 23, 11, 1391-400.
-
M. E. Thase. “Effects of venlafaxine on blood pressure: a meta-analysis of original data from 3744 depressed patients.” J. Clin. Psychiatry 1998, 59, 10, 502-08.
-
D. Nader, L. Gowing. “Is long-term benzodiazepine use a risk factor for cognitive decline? Results of a systematic review.” J. Addict. 2020, 2020, 1569456.
-
D. Cyranoski. “Why chinese medicine is heading for clinics around the world.” Nature 2018, 561, 7724, 448-50.
-
J. Wang, X. Xiong. “Evidence-based chinese medicine for hypertension.” Evid.-based Complement. Altern. Med. : eCAM 2013, 2013, 978398.
-
Z. Sun, Y. Xu, W. An, S. Bi, S. Xu, R. Zhang, M. Cong, S. Chen. “Mining important herb combinations of traditional chinese medicine against hypertension based on the symptom-herb network combined with network pharmacology.” Evid.-Based Complement. Altern. Med.: eCAM 2022, 2022, 5850899.
-
T. Yin, H. Zhang, X. Liu, D. Wei, C. Ren, L. Cui, Y. Li, L. Wang, J. Wang, Z. Zhao, D. Liu, L. Wang, X. Han. “Elucidating the anti-hypertensive mechanisms of uncaria rhynchophylla-alisma plantago-aquatica L: an integrated network pharmacology, cluster analysis, and molecular docking approach.” Front. Chem. 2024, 12.
-
Chinese Pharmacopoeia Commission. "Pharmacopoeia of the People’s Republic of China (Volume I, 2020 Edition)." China Medical Science Press, Beijing, 2020.
-
American Psychiatric Association. "Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5)." American Psychiatric Publishing, Arlington, VA, 2013.
-
M. Jiang, C. Lu, C. Zhang, J. Yang, Y. Tan, A. Lu, K. Chan. “Syndrome differentiation in modern research of traditional chinese medicine.” J. Ethnopharmacol. 2012, 140, 3, 634-42.
-
A. Lu, M. Jiang, C. Zhang, K. Chan. “An integrative approach of linking traditional chinese medicine pattern classification and biomedicine diagnosis.” J. Ethnopharmacol. 2012, 141, 2, 549-56.
-
M. Hamilton. “The assessment of anxiety states by rating.” Br. J. Med. Psychol. 1959, 32, 1, 50-55.
-
D. J. Buysse, C. F. Reynolds, T. H. Monk, S. R. Berman, D. J. Kupfer. “The pittsburgh sleep quality index: a new instrument for psychiatric practice and research.” Psychiatry Res. 1989, 28, 2, 193-213.
-
J. E. Ware, C. D. Sherbourne. “The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection.” Med. Care 1992, 30, 6, 473-83.
-
J. Wang, B. Feng, X. Yang, W. Liu, Y. Liu, Y. Zhang, G. Yu, S. Li, Y. Zhang, X. Xiong. “Tianma gouteng yin as adjunctive treatment for essential hypertension: a systematic review of randomized controlled trials.” Evid.-based Complement. Altern. Med. : eCAM 2013, 2013, 706125.
-
X.-J. Xiong, X.-C. Yang, W. Liu, L. Duan, P.-Q. Wang, H. You, X.-K. Li, S. Wang. “Therapeutic efficacy and safety of traditional chinese medicine classic herbal formula longdanxiegan decoction for hypertension: a systematic review and meta-analysis.” Front. Pharmacol. 2018, 9, 466.
-
W. Ren, M. Wang, J. Liao, L. Li, D. Yang, R. Yao, L. Huang. “The effect of chinese herbal medicine combined with western medicine on vascular endothelial function in patients with hypertension: a systematic review and meta-analysis of randomized controlled trials.” Front. Pharmacol. 2020, 11, 823.
-
W.-B. Zhang, C.-X. Chen, S.-M. Sim, C.-Y. Kwan. “In vitro vasodilator mechanisms of the indole alkaloids rhynchophylline and isorhynchophylline, isolated from the hook of uncaria rhynchophylla (miquel).” Naunyn-Schmiedeberg’s Arch. Pharmacol. 2004, 369, 2, 232-38.
-
P.-Y. Li, X.-R. Zeng, J. Cheng, J. Wen, I. Inoue, Y. Yang. “Rhynchophylline-induced vasodilation in human mesenteric artery is mainly due to blockage of L-type calcium channels in vascular smooth muscle cells.” Naunyn-Schmiedeberg’s Arch. Pharmacol. 2013, 386, 11, 973-82.
-
S. M. Hwang, Y. J. Lee, Y. P. Lee, J. J. Yoon, S. M. Lee, J. D. Cha, K. M. Choi, D. G. Kang, H. S. Lee. “Anti-proliferative effect of an aqueous extract of prunella vulgaris in vascular smooth muscle cells.” Evid.-based Complement. Altern. Med. : eCAM 2013, 2013, 936463.
-
M. Alexeev, D. K. Grosenbaugh, D. D. Mott, J. L. Fisher. “The natural products magnolol and honokiol are positive allosteric modulators of both synaptic and extra-synaptic GABA(a) receptors.” Neuropharmacology 2012, 62, 8, 2507-14.
-
V. Borgonetti, P. Governa, F. Manetti, E. Miraldi, M. Biagi, N. Galeotti. “A honokiol-enriched magnolia officinalis rehder & E.H. wilson. bark extract possesses anxiolytic-like activity with neuroprotective effect through the modulation of CB1 receptor.” J. Pharm. Pharmacol. 2021, 73, 9, 1161-68.
-
B. Huang, Y. Wu, C. Li, Q. Tang, Y. Zhang. “Molecular basis and mechanism of action of albizia julibrissin in depression treatment and clinical application of its formulae.” Chin. Herb. Med. 2023, 15, 2, 201-13.
-
B. Huang, H. Liu, Y. Wu, C. Li, Q. Tang, Y.-W. Zhang. “Two lignan glycosides from albizia julibrissin durazz. Noncompetitively inhibit serotonin transporter.” Pharmaceuticals 2022, 15, 3, 344.
-
L. Cai, R. Li, W. Tang, G. Meng, X. Hu, T. Wu. “Antidepressant-like effect of geniposide on chronic unpredictable mild stress-induced depressive rats by regulating the hypothalamus-pituitary-adrenal axis.” Eur. Neuropsychopharmacol.: J. Eur. Coll. Neuropsychopharmacol. 2015, 25, 8, 1332-41.
-
M. Wang, L. Yang, Z. Chen, L. Dai, C. Xi, X. Wu, G. Wu, Y. Wang, J. Hu. “Geniposide ameliorates chronic unpredictable mild stress induced depression-like behavior through inhibition of ceramide-PP2A signaling via the PI3K/akt/GSK3β axis.” Psychopharmacology (Berl.) 2021, 238, 10, 2789-800.
-
C. Cheng, T. Wu, H. Shang, Y. Li, D. G. Altman, D. Moher, Z. Bian, For The Consort-Chm Formulas 2017 Group. “CONSORT extension for chinese herbal medicine formulas 2017: recommendations, explanation, and elaboration.” Ann. Intern. Med. 2017, 167, 2, 112-21.