Research Progress in System Construction and Image Processing Algorithms of Optical Coherence Tomography (OCT)
Abstract
As a non-invasive, high-resolution tomographic imaging technique based on the principle of low-coherence interferometry, Optical Coherence Tomography (OCT) has established a pivotal position in biomedical clinical diagnosis, industrial non-destructive testing and other fields. The core trajectory of its technological evolution is manifested in the shift from the time domain to the Fourier domain. In particular, Spectral Domain OCT (SD-OCT) and Swept Source OCT (SS-OCT) have achieved an order-of-magnitude improvement in imaging speed and sensitivity by virtue of their parallel detection architecture. The current development of OCT technology has always revolved around two core dimensions: system hardware construction and image processing algorithms. At the hardware level, existing technologies have achieved continuous optimization of resolution and imaging depth, but have been unable to break through the intrinsic constraints of core performance under the classical optical framework; at the algorithm level, the technical system has completed the transformation from model-driven to data-driven, yet still faces the core bottleneck of translating laboratory performance into clinical practical value. This paper systematically reviews the research progress of OCT system construction and image processing algorithms, deeply analyzes the unsolved core bottlenecks in the two dimensions, clarifies the core path of future technological breakthroughs, and provides a reference for the basic research and clinical translation of OCT technology.
1. Introduction
Optical Coherence Tomography (OCT) is a novel three-dimensional (3D) imaging technology first proposed by Huang et al. in 1991[1]. The physical basis of OCT lies in low-coherence interferometry. By analyzing the backscattered signals of broadband light from the microstructures inside the sample, it realizes high-resolution, non-invasive tomographic imaging of transparent or scattering media such as biological tissues[2,3]. Since its inception, the technical path has undergone fundamental transformations: from Time-Domain OCT (TD-OCT) (as shown in Figure 1), which relies on mechanical scanning of the reference arm for depth encoding, to Frequency-Domain OCT (FD-OCT), which directly extracts depth information through Fourier analysis of interference spectra. This shift, especially its two main practical branches—Spectral-Domain OCT (SD-OCT) based on camera-captured spectra and Swept-Source OCT (SS-OCT) based on rapidly tunable lasers (as shown in Figure 2), has brought about orders-of-magnitude improvements in imaging speed and detection sensitivity, laying the foundation for the application of OCT in dynamic in vivo imaging[4-7].
Today, the application boundary of OCT has far exceeded the field of ophthalmology. It has shown great potential in biomedical scenarios such as cardiovascular endoscopic imaging, early gastrointestinal cancer screening, skin disease diagnosis, and intraoperative monitoring in neurosurgery. Meanwhile, it has achieved large-scale application in cross-cutting fields including industrial welding quality monitoring (as shown in Figure 3), material non-destructive testing, forensic science evidence analysis, and cultural relic disease assessment[8-12]. The continuous expansion of application scenarios has put forward higher requirements for the core performance, scenario adaptability and clinical usability of OCT technology, and also highlights two unavoidable core contradictions in the current technological development, which are the two core points of this paper:
The first core point: At the level of OCT system construction, existing technologies have achieved an order-of-magnitude breakthrough in core indicators such as axial resolution and imaging depth through iterative optimization of light sources, spectrometers, scanning mechanisms and integrated architectures. However, they can never fundamentally break the inherent inverse relationship between resolution and imaging depth under the classical optical framework. At the same time, they fail to solve the core bottlenecks including the attenuation of sensitivity with imaging depth, the difficulty in balancing high performance with system miniaturization and low cost, and the mismatch between technical indicators and clinical needs[13,15]. Existing engineering optimization can only alleviate the contradictions, but cannot achieve essential breakthroughs. In the future, it is possible to break through the limitations of the traditional technical framework and realize the simultaneous breakthrough of core performance and scenario adaptability through the innovation of new physical principles, chip-level integrated optics, software-hardware co-design and other means.
The second core argument: At the level of OCT image processing, the algorithm system has completed the paradigm shift from classical statistical model-driven to deep learning data-driven, and has achieved leapfrog development in speckle noise suppression, image super-resolution enhancement, functional information extraction, and intelligent disease diagnosis. However, existing algorithms have always been unable to solve the exclusive pain points brought by the physical characteristics of OCT coherent imaging. There are core problems including the disconnection between physical priors and algorithm models, the mismatch between algorithm optimization objectives and clinical diagnosis needs, and the insufficient coordination between hardware performance and algorithm capabilities, which make it difficult to translate the excellent laboratory performance into stable clinical practical value[16-19]. In the future, it is possible to promote the leap of algorithms from "indicator optimization" to "clinical availability" through solutions such as explainable AI embedded with physical priors, self-supervised learning, and software-hardware collaborative optimization.
This paper will focus on the above two core points, take system hardware construction and image processing algorithms as the two main chapters, systematically sort out the research progress of OCT technology, deeply analyze the core bottlenecks and unsolved problems of existing technologies, and put forward the corresponding future breakthrough paths and development directions.
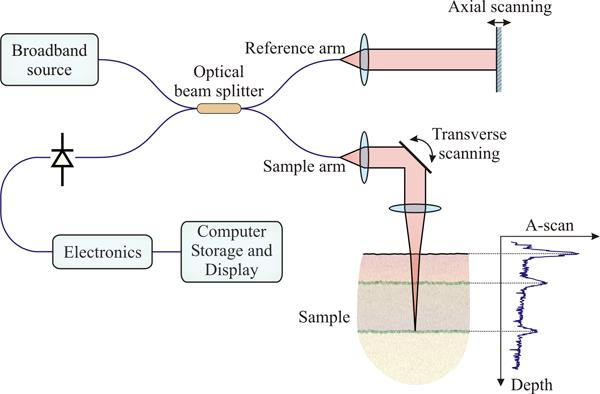
Figure 1. Schematic diagram of the basic structure of Time-Domain OCT, showing axial depth encoding by mechanical scanning of the reference arm. Adapted from Ref. [29]
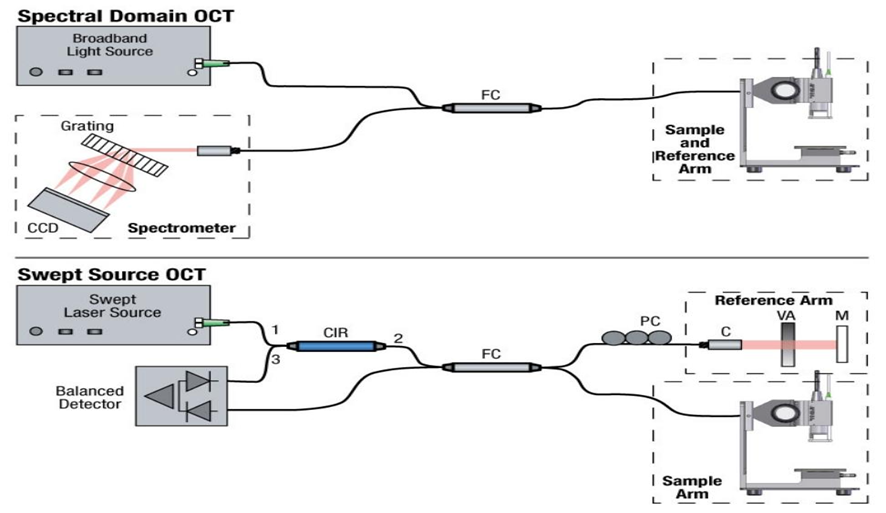
Figure 2. Comparison of the basic structures of SD-OCT and SS-OCT, illustrating spectrometer-based spectral acquisition and swept-source wavelength scanning. Adapted from Ref. [29]
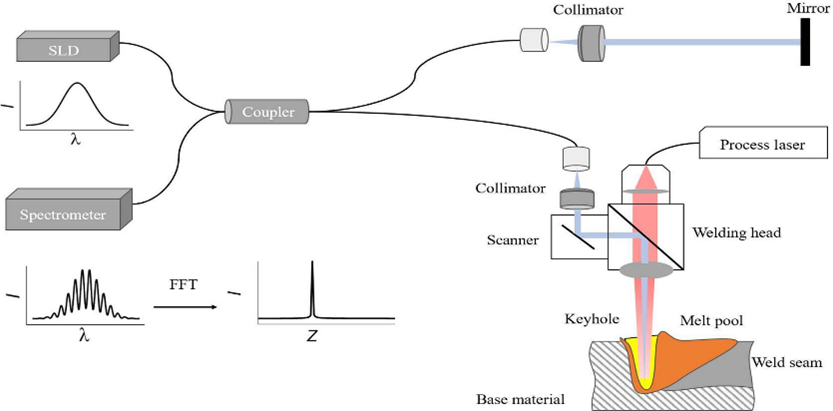
Figure 3. Schematic of the welding depth measurement system based on SD-OCT, showing how tomographic signals are used to monitor weld/keyhole geometry during laser processing. Adapted from Ref. [9]
2. Research on Design and Implementation Methods of Spectral-Domain OCT Systems
2.1. Technical Progress in OCT System Construction for Core Performance Optimization
2.1.1. Light Source and Spectrometer
The light source is the physical origin of OCT system performance. Its central wavelength mainly affects the tissue penetration depth and scattering characteristics, while the spectral bandwidth directly determines the ultimate axial resolution of the system, but there is an inverse relationship between the two[20]. To pursue sub-micron or even higher resolution, ultra-broadband light sources such as supercontinuum sources have been widely adopted. For example, in 2004, Barry Cense and Nader A. Nassif achieved 4 μm axial resolution by splicing two SLD light sources, which has obvious advantages in cost and system construction, but the resolution improvement is limited; in the same year, N. A. Nassif's team developed an SD-OCT system that achieved 6 μm axial resolution in the retina and a maximum sensitivity of 98.4 dB, and its fast 3D imaging capability can clearly present retinal structures, but the field of view is relatively small (as shown in Figure 4)[21]; in 2009, V. J. Srinivasan's team achieved ≈3.3 μm axial resolution in tissues based on ultra-high-resolution OCT with a 50 kHz A-line rate, which can be used to detect retinal functional responses, but the field of view is small and usually needs to be combined with noise reduction processing[22]; in 2013, Lin An's team launched a 1050 nm SD-OCT system with an axial resolution of ≈10 μm in air and an imaging depth of 6.1 mm, which has the advantages of large imaging depth and wide field of view, but the resolution is relatively low (as shown in Figure 5)[23]; in 2020, ByungKun Lee's team developed an 840 nm UHR SD-OCT with an axial resolution of 2.4 μm (unshaped spectrum)/2.7 μm (spectral shaping) in tissues, which can clearly display the fine structures of tissues, but the resolution slightly decreases after spectral shaping (as shown in Figure 6)[24]; in 2025, Mohammad Hossein Vafaie's team designed a UHR SD-OCT for retinal applications, with an axial resolution ≤3 μm, a lateral resolution ≤15 μm, and a maximum imaging depth ≥1.5 mm. Its parameters are specially optimized for retinal imaging, but the clinical effect of the system remains to be further verified[25]. Another mainstream technical path—Swept-Source OCT (SS-OCT)—obtains depth information mainly by rapidly and continuously tuning the laser wavelength. In recent years, swept-source OCT has also achieved extensive development and application. Among them, Micro-Electro-Mechanical System (MEMS)-based Vertical-Cavity Surface-Emitting Lasers (MEMS-VCSEL) have become an important choice for commercial ophthalmic OCT systems due to their good balance between sweep rate, cost, and reliability[14,26].
Both system sensitivity and resolution are important indicators to measure the system. Among them, the Relative Intensity Noise (RIN) of the light source is one of the key factors limiting system sensitivity. Using semiconductor optical amplifiers for gain saturation amplification or designing multi-channel detection to average noise are effective suppression strategies[27,28].
In SD-OCT, the spectrometer, as the core component that converts interference spectral signals into digital information, its performance is crucial (as shown in Figure 7(a)). Spectrometers face many challenges, such as system sensitivity attenuation and noise control, dispersion mismatch and compensation, system stability and calibration, etc. Among them, the problem of system sensitivity attenuation lies in realizing the linear mapping from spectrum to wavenumber space to mitigate nonlinear sampling. Nowadays, there are many methods to alleviate this problem. For example, the linear wavenumber spectrometer design combining prisms and diffraction gratings can effectively reduce errors caused by interpolation in data processing, becoming the mainstream scheme for high-performance systems[20,29]. In addition, there are some innovative designs, such as constructing an orthogonal dispersion spectrometer by combining gratings with Virtual Image Phase Array (VIPA), which can achieve high spectral resolution while covering a wide free spectral range, providing possibilities for long-distance and high-precision measurements (as shown in Figure 7(b))[30].
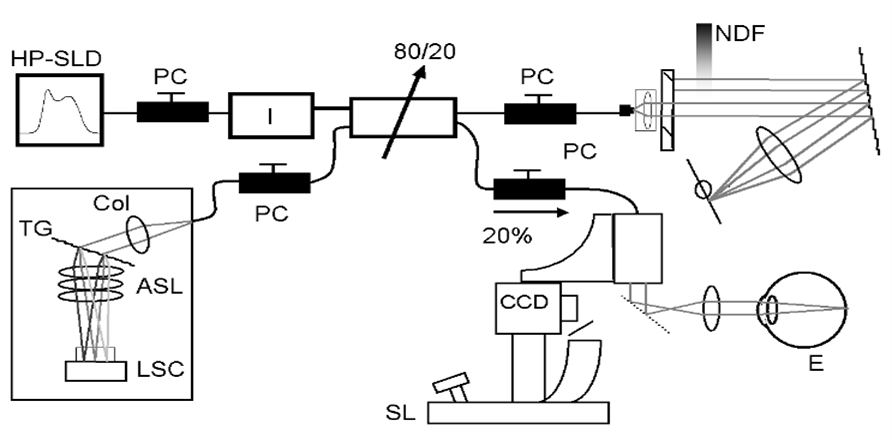
Figure 4. Spectral-domain OCT setup for retinal imaging. The system includes a high-powered superluminescent diode source (HP-SLD), polarization controllers (PC), slit-lamp (SL), neutral density filter (NDF), collimator (Col), transmission grating (TG), air-spaced focusing lens (ASL), linescan camera (LSC), and the eye, illustrating the spectral-interferometric acquisition pathway. Adapted from Ref. [21]
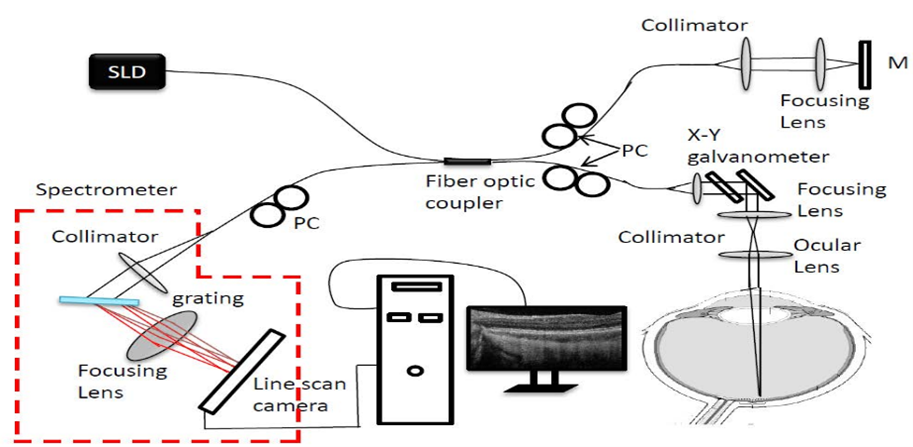
Figure 5. Schematic of the ultrahigh-speed SD-OCT system setup, showing the 1.0 µm SLD source, polarization controller (PC), reference mirror (M), and optical path used for high-speed deep retinal imaging. Adapted from Ref. [23]
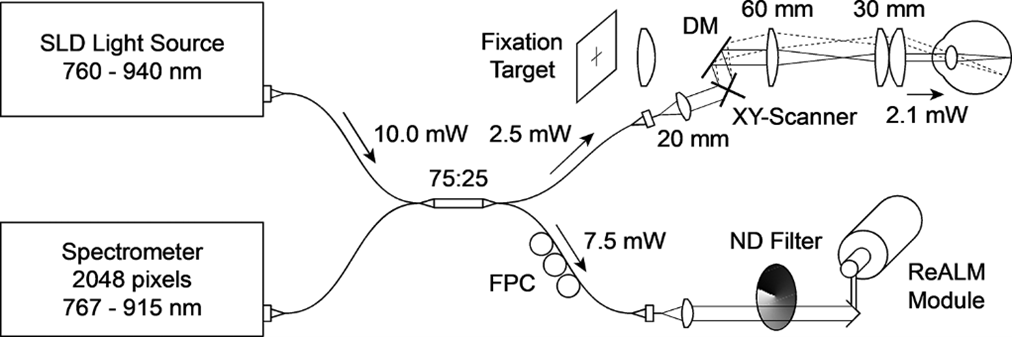
Figure 6. Schematic diagram of the UHR SD-OCT system, showing spectral shaping to balance higher axial resolution and longer imaging range. DM, dichroic mirror; FPC, fiber polarization controller; ND, neutral density; SLD, superluminescent diode. Adapted from Ref. [24]
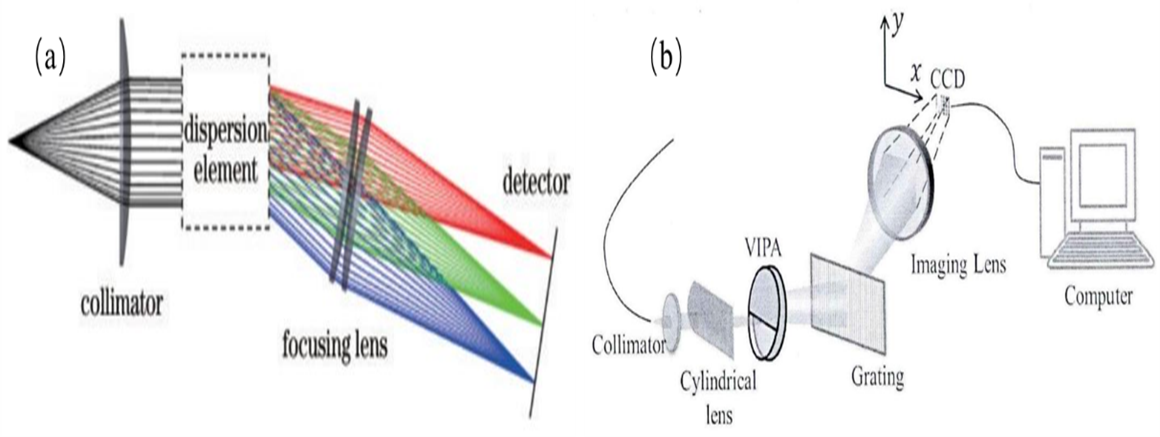
Figure 7. (a) General structure of the spectrometer used for spectral sampling in SD-OCT. (b) Orthogonal dispersive spectrometer structure, illustrating a design route for improving spectral resolution and free spectral range. Adapted from Refs. [29,30]
2.1.2. Scanning Mechanism and System Architecture
The ability to achieve fast and accurate lateral scanning is the basis for acquiring 2D and 3D images and a key to system miniaturization. For miniaturization, traditional galvanometer scanners are gradually being replaced by more compact and fast Micro-Electro-Mechanical System (MEMS) mirrors. However, MEMS mirrors also have certain problems. To address the inherent nonlinearity and scanning distortion of electrothermally driven MEMS mirrors, studies have proposed an open-loop feedforward control algorithm based on their transfer function. By optimizing the driving voltage waveform, it effectively corrects fan-shaped distortion and significantly improves the geometric fidelity of imaging[31]. Revolutionary non-mechanical scanning schemes are also emerging. For example, using the electrowetting effect to control the curvature of the interface between two immiscible liquids to form a voltage-tunable prism, realizing extremely compact beam deflection, which is very suitable for scenarios with strict space requirements such as endoscopes[32]. In terms of invasive imaging, the all-optical driven MEMS fiber endoscope probe (as shown in Figure 8) transmits driving light through optical fibers and converts it into voltage at the distal end to drive the MEMS mirror, completely avoiding electromagnetic interference and patient safety risks caused by electrical connections, showing extremely high clinical application potential and bringing many benefits for subsequent medical applications[33].
The design of the system architecture needs to be closely centered on the requirements of specific application scenarios. To meet the clinical examination needs of special populations such as bedridden patients and infants, a portable cantilever-type OCT system supporting supine operation has emerged (as shown in Figure 9). Such systems integrate real-time iris imaging and electric focusing functions (as shown in Figure 10), greatly improving the success rate of high-quality retinal imaging in challenging body positions[34]. For unstable environments such as handheld or endoscopic imaging, the common-path interference architecture integrates the reference reflection surface into the sample arm probe, making a part of the sample arm beam itself serve as the reference light, which greatly enhances the system's ability to resist environmental vibration interference[35,36]. In addition, the innovative dual-interferometer design combined with a single spatial light modulator realizes independent and precise regulation of the wavefronts of the reference arm and sample arm, providing a powerful tool for optimizing focusing and improving signal intensity at specific depths in strongly scattering media[37].
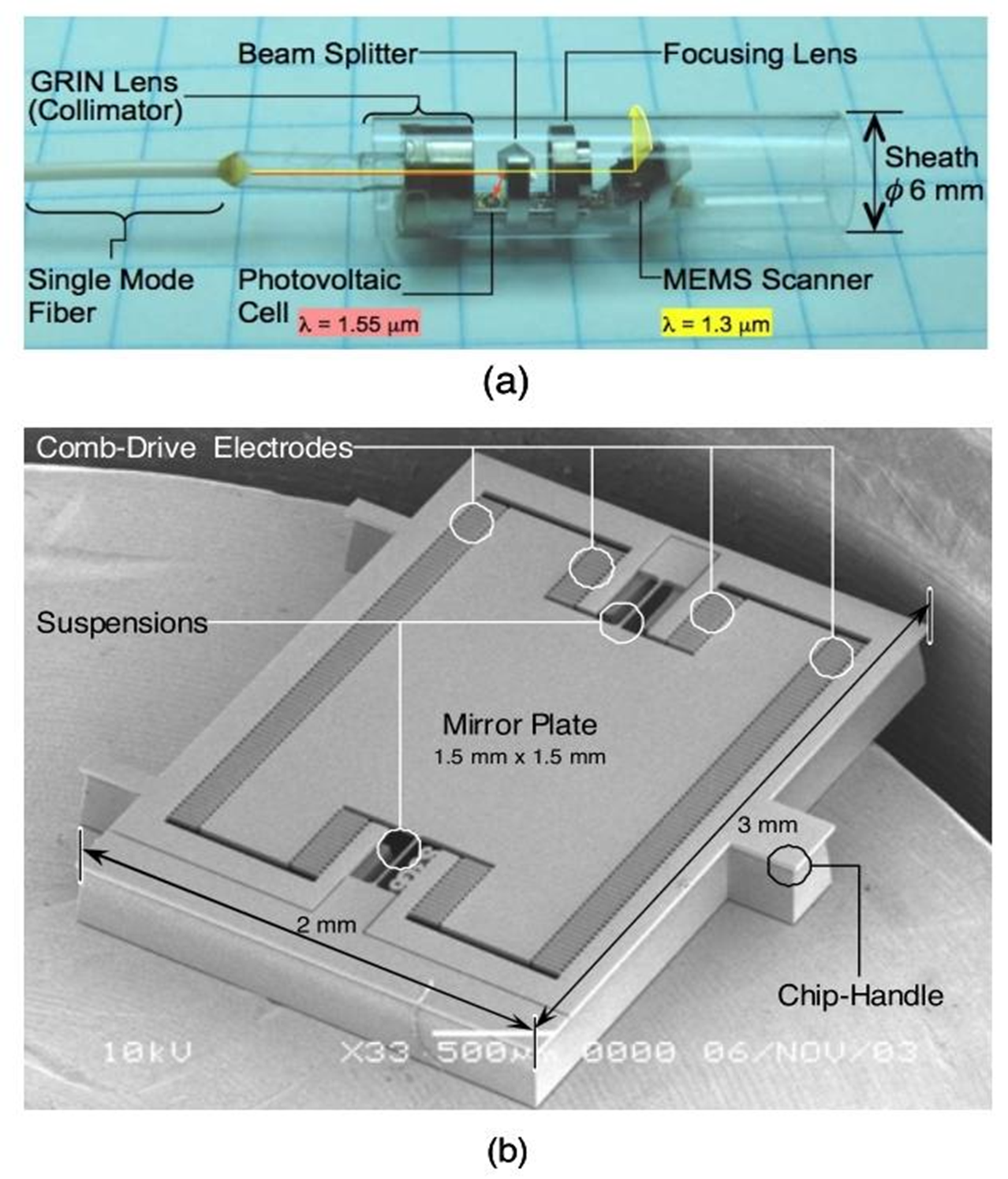
Figure 8. Photographs of the MEMS optical endoscope. (a) Probe assembly with the input/output fiber, lens optics, and MEMS scanner. (b) SEM image of the electrostatic MEMS optical scanner, illustrating distal beam steering for endoscopic OCT. Adapted from Ref. [33]
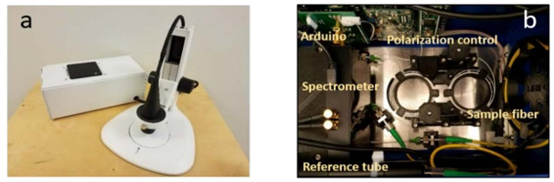
Figure 9. Low-cost portable OCT system. (a) System engine. (b) Top view of the system interior, illustrating compact integration for point-of-care imaging. Adapted from Ref. [15]
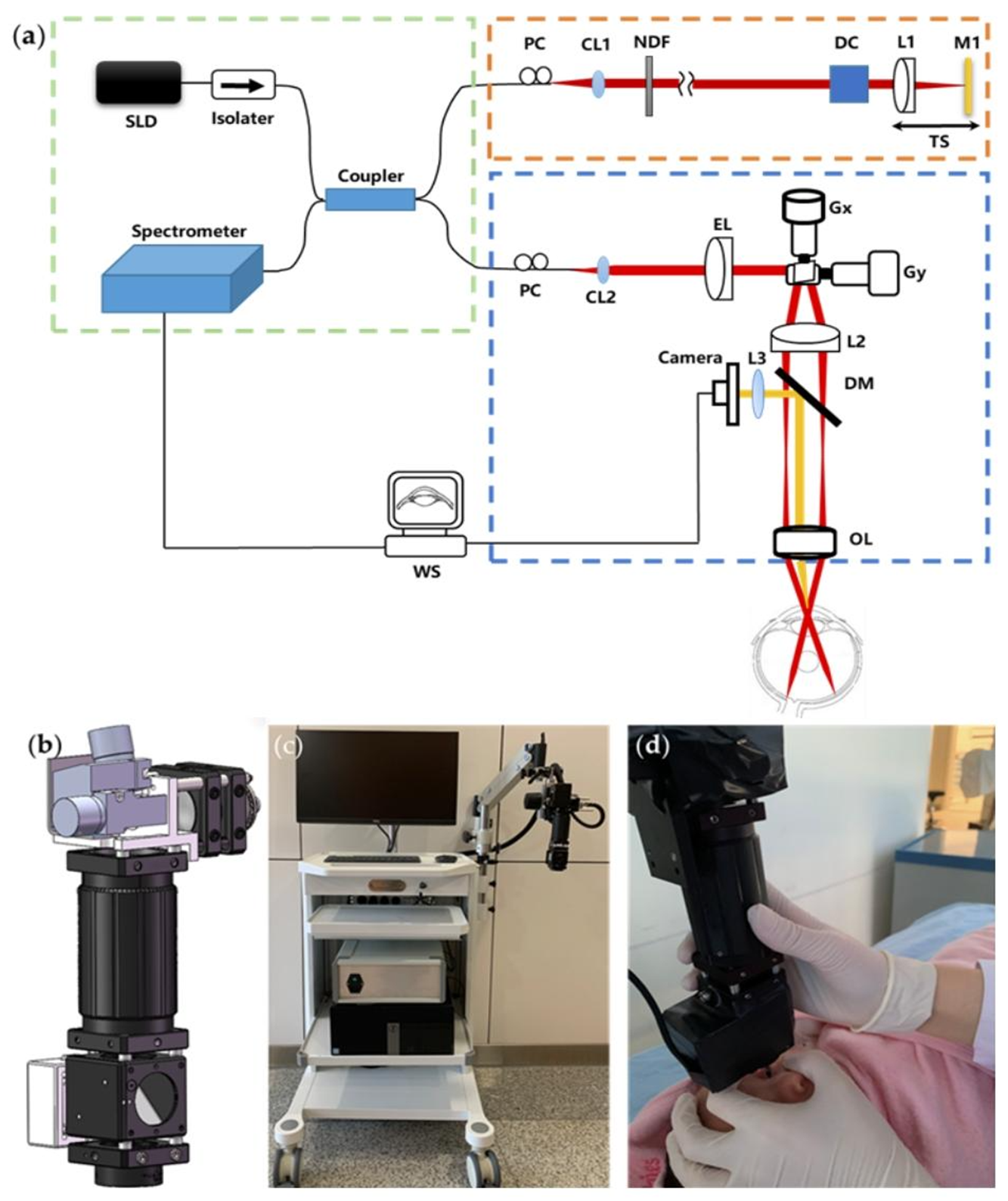
Figure 10. Schematic and photo of the portable boom-type UHR-OCT for supine retinal imaging. (a) System schematic; SLD, superluminescent diode; CL, collimator; NF, neutral-density filter; DC, dispersion compensation prisms; L, lens; G, galvanometer scanner; TS, translational stage; WS, workstation; EL, electronically tunable lens; PC, polarization controller; DM, dichroic mirror; BS, beam splitter; OL, ocular lens. (b) Main components of the probe. (c) Photograph of the system. (d) Clinical imaging of an infant, showing the workflow enabled by the portable boom-type configuration. Adapted from Ref. [34]
2.2. Core Bottlenecks and Future Breakthrough Paths of OCT System Construction
Although existing OCT system construction technologies have achieved an order-of-magnitude breakthrough in core indicators such as resolution and imaging depth through the iteration of core devices and architectures, there are still four core bottlenecks restricting its essential technological breakthrough and large-scale clinical implementation:
First, it is impossible to break the inherent physical contradiction between resolution and imaging depth under the classical optical framework. Under the classical optical framework, the axial resolution of OCT is determined by the spectral bandwidth of the light source, satisfying the formula Δz=(2ln2/π)(λ₀²/Δλ), where λ₀ is the central wavelength of the light source and Δλ is the spectral bandwidth. Resolution and penetration depth are inversely related via the central wavelength and spectral bandwidth of the light source. A long wavelength can improve the tissue penetration depth but will reduce the lateral resolution, and the realization of ultra-broad spectral bandwidth in the long wavelength band has device technical barriers, making it impossible to achieve simultaneous optimal improvement of the two in a single system.
Second, it is impossible to completely eliminate the attenuation of sensitivity and resolution with imaging depth. The increase in imaging depth will lead to an exponential attenuation of the backscattered signal of the sample, superimposed with problems such as nonlinear sampling of the spectrometer and dispersion mismatch, which further aggravate the performance degradation. Existing compensation and optimization schemes can only alleviate this problem, but cannot fundamentally reverse the signal-to-noise ratio attenuation in deep imaging.
Third, it is difficult to balance the trade-off between high performance and system miniaturization, low cost, and clinical adaptability. High-performance systems rely on high-end optoelectronic devices, which have the problems of large volume, high cost, and high operation threshold, making it difficult to popularize in primary healthcare. In contrast, low-cost portable systems sacrifice core imaging performance to compress volume and cost, which cannot meet the needs of high-precision clinical diagnosis, resulting in a serious mismatch with the actual clinical scenario needs.
Fourth, the problem of motion distortion and artifacts in dynamic in vivo imaging cannot be effectively solved. Random physiological movements such as heartbeat, respiration, and gastrointestinal peristalsis lead to reduced image resolution and structural dislocation. Existing scanning optimization schemes can only correct the inherent distortion of the scanning mechanism, and cannot realize real-time and accurate compensation for the random movement of living tissues.
In view of the above core bottlenecks, combined with the development trend of optical engineering and integrated photonics technology, the essential breakthrough of OCT system construction can be achieved through four core paths in the future:
First, by relying on new photonic devices such as metasurface lenses, quantum light sources, and single-photon detectors, we can break the inherent limitation between resolution and imaging depth in terms of physical principles, and improve the detection efficiency of weak signals in deep imaging[38].
Second, by realizing the full link integration of the chip-level OCT system based on silicon-based and silicon nitride photonic platforms, we can greatly reduce the system volume and cost, reduce the optical path loss, dispersion mismatch and other problems caused by discrete devices, and fundamentally improve the stability and consistency of the system.
Third, by adopting scenario-customized design, getting rid of the development path of indiscriminately pursuing the ultimate indicators, directionally optimizing system parameters and architecture for different scenarios such as ophthalmology, cardiovascular endoscopy, and primary medical screening, we can break the inherent contradiction between performance and cost, and realize the precise matching of technology and clinical needs.
Fourth, by constructing a closed-loop system of "scanning-acquisition-correction" through software-hardware collaborative optimization, combining the real-time processing capability of Field Programmable Gate Array (FPGA) and new non-mechanical scanning technology, we can realize full-link real-time motion compensation for dynamic in vivo imaging, and fundamentally solve the artifact problem of dynamic imaging[39].
3. Research Progress in OCT Image Processing and Algorithms
3.1. Technological Evolution and Research Progress of OCT Image Processing Algorithms
3.1.1. Speckle Noise Suppression
Speckle noise, an inherent physical phenomenon in coherent imaging, presents as multiplicative, spatially correlated granular textures, which seriously interfere with image interpretation and quantitative analysis[38-41]. Early suppression methods mainly relied on modeling the statistical characteristics of noise or images, including anisotropic diffusion filtering based on local statistics, wavelet threshold denoising using multi-scale and multi-directional analysis, and dictionary learning algorithms based on image patch sparse representation[42-44]. Although these methods have physical interpretability, they often face an irreconcilable contradiction between noise suppression and preservation of fine tissue structures.
The rise of deep learning has brought a paradigm revolution to speckle suppression. Supervised learning methods, such as Denoising Convolutional Neural Networks (DnCNN), perform end-to-end training through a large number of "noisy-clean" image pairs, which can effectively learn the complex mapping from noisy images to potentially clear images, achieving performance significantly superior to traditional methods[16,45]. Given the difficulty in obtaining absolutely "clean" label data in the medical field, unsupervised or self-supervised learning has become a research hotspot. For example, by sampling multiple sub-patches from a single noisy image to construct self-supervised training pairs, or designing a triplet cross-fusion learning strategy to train using unpaired noisy and relatively clean images, these methods can achieve denoising effects comparable to supervised learning without ideal labels[46,47]. Generative Adversarial Networks (GANs) can generate results visually closer to real tissue textures[48], while emerging diffusion models learn the inverse process by simulating complex noise degradation processes, showing unique advantages in detail preservation[49]. These advanced algorithms can usually increase the peak signal-to-noise ratio of images by several decibels and the structural similarity index by more than 0.1, effectively suppressing noise while better preserving crucial anatomical details.
Over the past two decades, OCT speckle noise suppression technology has undergone a profound evolution from model-driven to data-driven, and from general processing to specialized intelligence. In 2007, Salinas and Fernández introduced PDE-based nonlinear diffusion methods into OCT (as shown in Figure 11) laying the foundation for adaptive edge-preserving denoising, but they are parameter-sensitive and have limited suppression of multiplicative noise. Subsequently, software algorithms developed rapidly in the direction of improving intelligence and efficiency[50]; in 2013, Fang et al.'s sparse representation simultaneous denoising and interpolation framework achieved high-quality reconstruction from undersampled data, greatly improving the potential imaging speed, but it is computationally complex and relies on a large number of paired training datasets[51]; in 2015, Gong et al.'s adaptive total variation model better balanced denoising and edge preservation by dynamically adjusting the smoothing intensity (as shown in Figure 12)[52]; in 2017, Fang's team's segmentation-based sparse reconstruction method significantly improved reconstruction accuracy by training specialized dictionaries for each layer of the retina, but it is highly dependent on accurate segmentation results[53]. At the same time, the hardware path provides a simple parallel scheme, such as real-time speckle averaging using an optical chopper adopted by researchers in 2020, which is low-cost and easy to integrate, but introduces light loss and is sensitive to sample motion[54] . To promote the practical application of algorithms, in 2022, Li et al. achieved efficient adaptation of sparse representation methods through pre-trained global dictionaries and fast noise estimation (as shown in Figure 13)[44]; in 2023, You et al. represented in-depth tuning for specific tasks through systematic optimization of wavelet denoising parameters[55]. The latest frontier breakthroughs are reflected in the overcoming of clinical data bottlenecks by deep generative models: in 2025, Liu et al.'s proposed unpaired reference-guided generative adversarial network innovatively extracts high-frequency perturbations from real noisy images to construct training data pairs, which can effectively remove complex mixed noise in cellular-resolution OCT without simulating noise or acquiring demanding paired data, but its performance is still affected by the quality of reference images and there is a risk of domain shift (as shown in Figure 14)[56]. The THFN-OCT model proposed in 2025 represents the further intelligent development of diffusion models in this field. Based on the cold diffusion framework, this method explicitly encodes the time steps of the diffusion process into dynamic weights through frequency-domain decoupling and time-step-aware attention mechanisms, guiding the network to adaptively reconstruct low-frequency structures and enhance high-frequency details in different denoising stages. Its designed frequency-selective skip connections (FreqSkip) further alleviate the loss of high-frequency information caused by pooling and upsampling. Experiments show that the model achieves performance superior to existing methods on both public and private datasets, effectively suppressing noise while better preserving the fine structures and textures of the retina, promoting OCT denoising technology toward higher fidelity and stronger adaptability[49]. Looking at this course, technological development has always centered on the core trade-off of "denoising-fidelity-efficiency-feasibility". The latest research is committed to promoting OCT from a high-quality imaging tool to a fast, quantitative intelligent analysis platform that can solve practical clinical data problems through the combination of software and hardware and more intelligent algorithms.
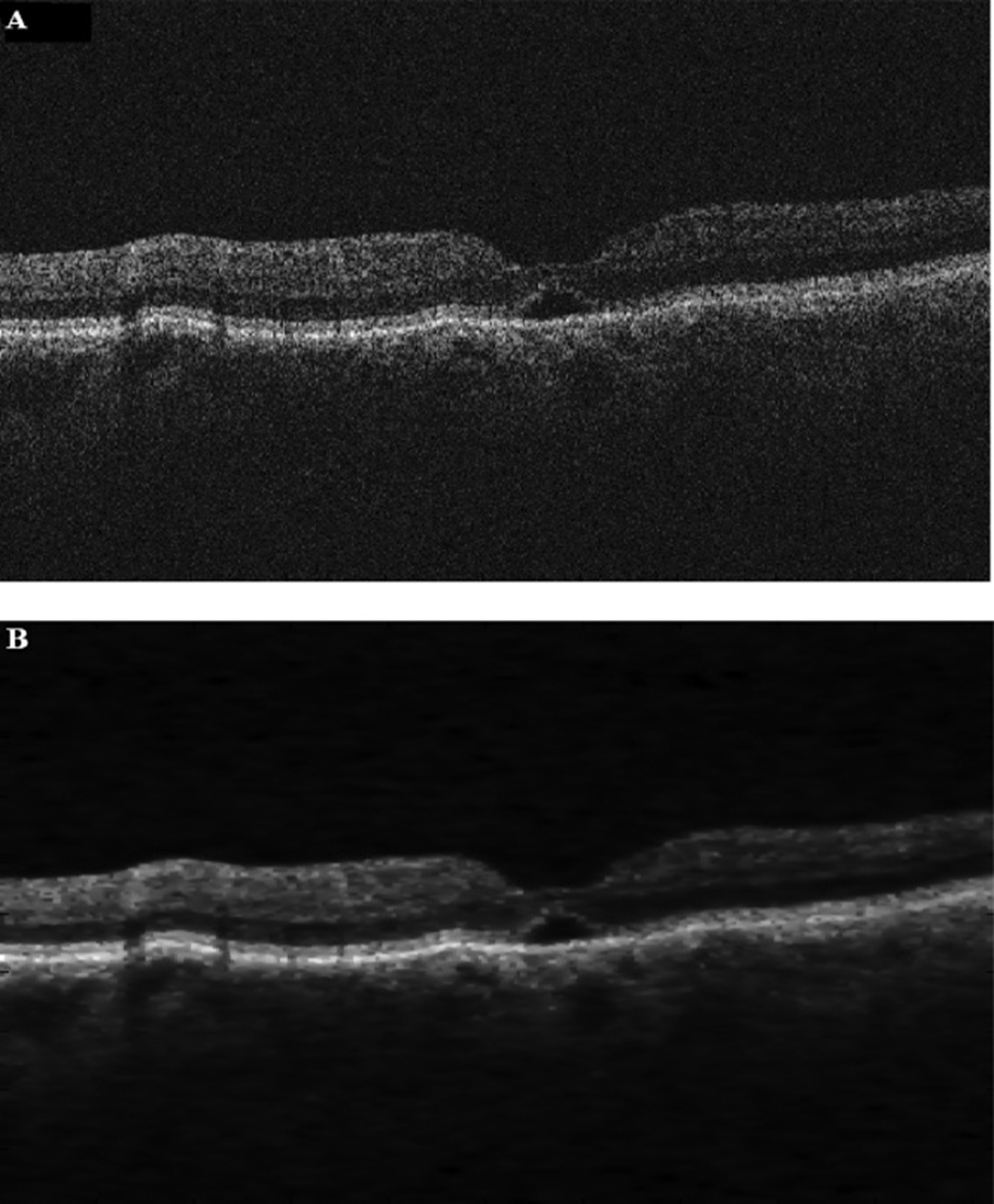
Figure 11. Experimental results on OCT images of patients with subfoveal cysts. (A) Noisy OCT image of the pathological sample. (B) Image denoised by the nonlinear complex diffusion filter, demonstrating edge-preserving speckle suppression. Adapted from Ref. [50]
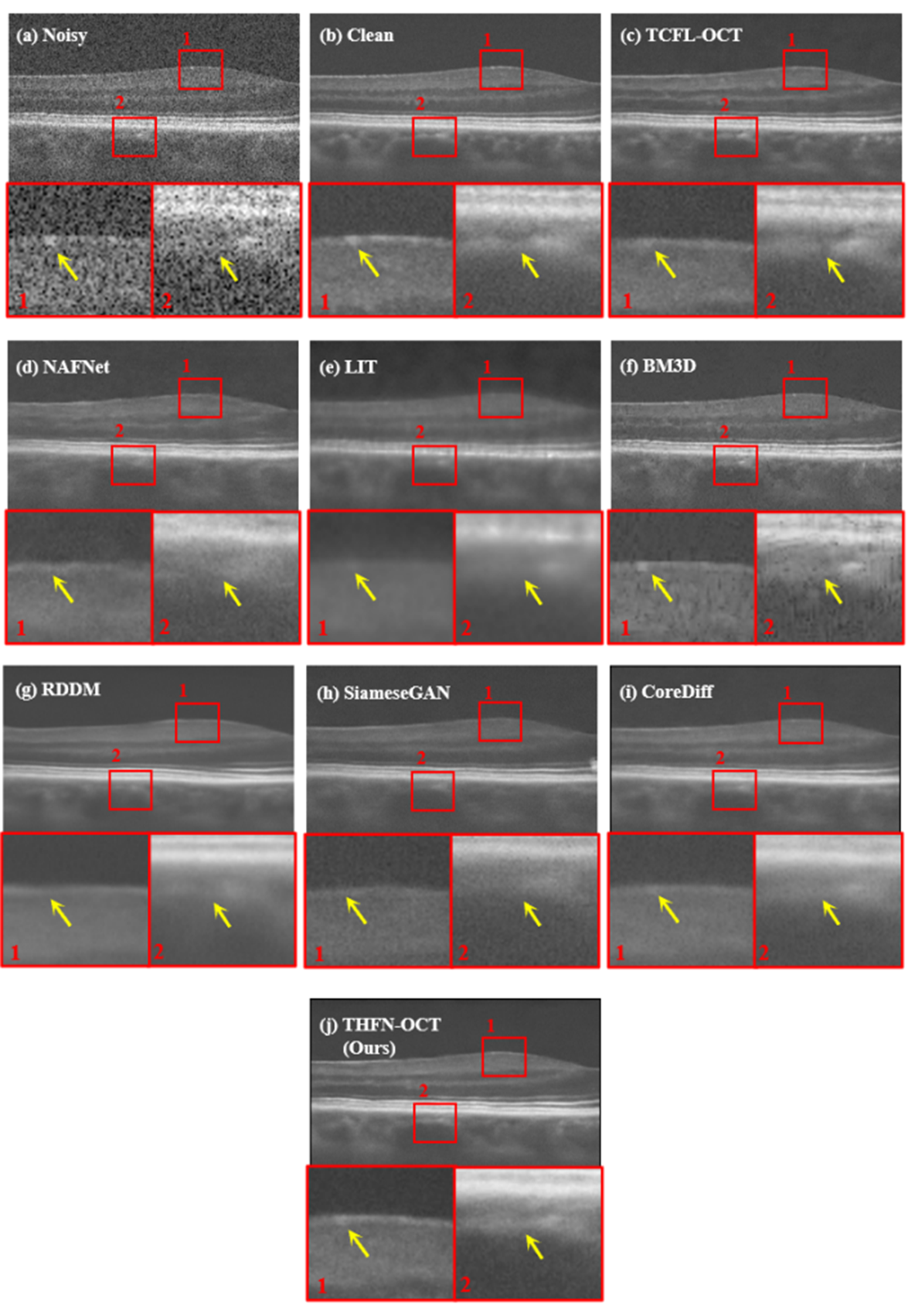
Figure 12. Comparison of denoising performance of different methods on the Duke-2013 dataset, illustrating the trade-off between speckle suppression and preservation of retinal structure. Adapted from Ref. [52]
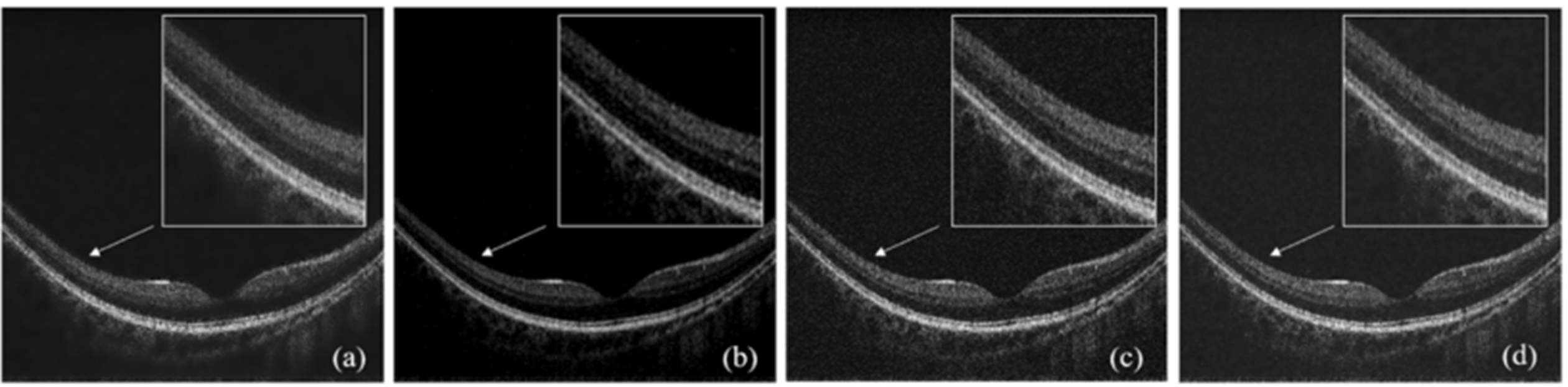
Figure 13. OCT images processed by different denoising methods: (a) 2D adaptive Wiener filtering; (b) wavelet soft-threshold denoising; (c) total variation (TV) denoising; (d) sparse representation, highlighting differences in noise suppression and structural retention. Adapted from Ref. [44]
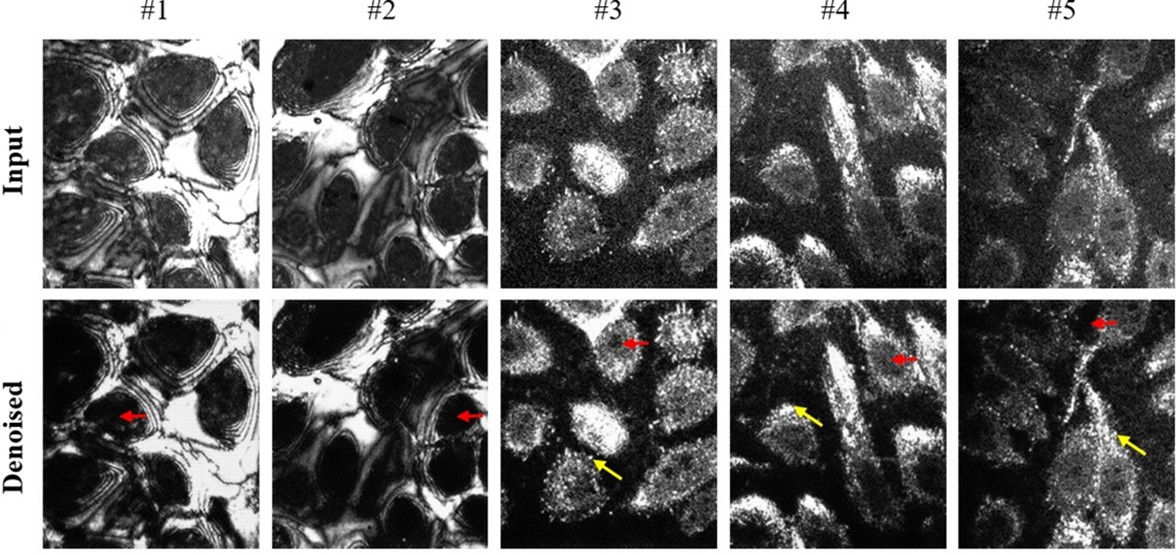
Figure 14. Denoising results of in vivo human skin images acquired by the visible-light source D-FF-OCT system. First row: original images. Second row: denoised images, showing the removal of mixed noise while preserving cellular-level structures. Adapted from Ref. [56]
3.1.2. Image Enhancement, Super-Resolution and Functional Expansion
Beyond simple noise suppression, algorithms aimed at actively improving image visual quality and information density are another active direction. To address image blurring caused by defocus or system aberrations, deep learning-based digital refocusing technology offers an effective solution. It can directly recover clear structures at the focal plane from a single defocused image, thereby effectively expanding the usable depth of field of the system and expanding the imaging range while ensuring resolution[57]. There are more complex computational optical methods, such as a joint optimization algorithm combining non-local self-similarity priors and Rayleigh-Sommerfeld diffraction models, which can even achieve image sharpening and artifact correction within a range far exceeding the traditional optical depth of field[58]. For improving spatial resolution, a one-dimensional deconvolution network based on deep learning can adaptively recover image details by inputting point spread function information, achieving an average lateral resolution improvement of approximately 23%[59]; while the technology combining multi-angle scanning and computational reconstruction, Optical Coherence Refraction Tomography (OCRT) (as shown in Figure 15), fundamentally breaks through the diffraction limit, achieving an order-of-magnitude improvement in lateral resolution and isotropic 3D imaging[60].
The great value of OCT lies more in its ability to expand functions beyond structural imaging. Optical Coherence Tomography Angiography (OCTA) generates high-resolution microvascular network images of the retina, choroid, and even skin by analyzing signal changes caused by red blood cell movement between consecutive B-scans without injecting exogenous contrast agents. It has become a core tool for the diagnosis and follow-up of vascular diseases such as diabetic retinopathy and age-related macular degeneration[61]. The core of its algorithm lies in the high-specificity separation of dynamic blood flow signals from static tissue backgrounds. New algorithms such as complex correlated phase gradient variance effectively improve the ability to resist artifacts such as eye movement and the specificity of blood flow detection by utilizing the stability of phase information[17]. Optical Coherence Elastography (OCE) can quantitatively map the biomechanical properties of tissues by detecting tiny deformations or vibrations of tissues under internal or external mechanical stimulation, providing a new dimension for the differential diagnosis of tumors and the evaluation of corneal biomechanics (as shown in Figure 16)[62]. The development of this technology is closely dependent on high-precision displacement estimation technology and supporting image quality evaluation standards[63,64].
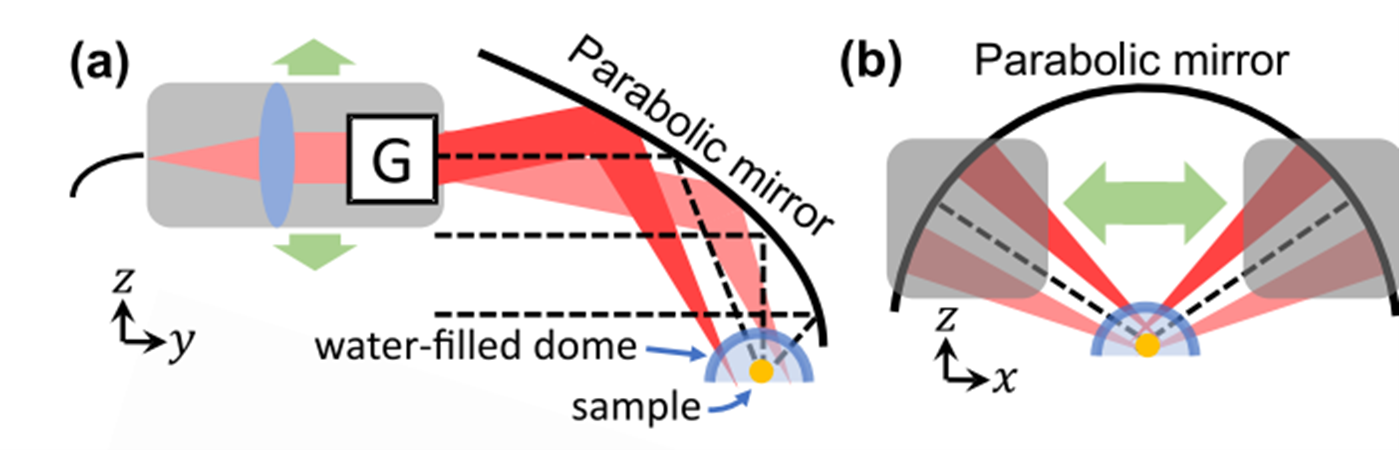
Figure 15. Parabolic-mirror-based OCRT imaging system enabling multi-view imaging over wide angular ranges. (a,b) Schematic of the imaging system, in which a 2D translating probe angularly scans a collimated beam with galvanometers (G), and the sample is placed at the center of a water-filled glass optical dome for computational 3D reconstruction. Adapted from Ref. [60]
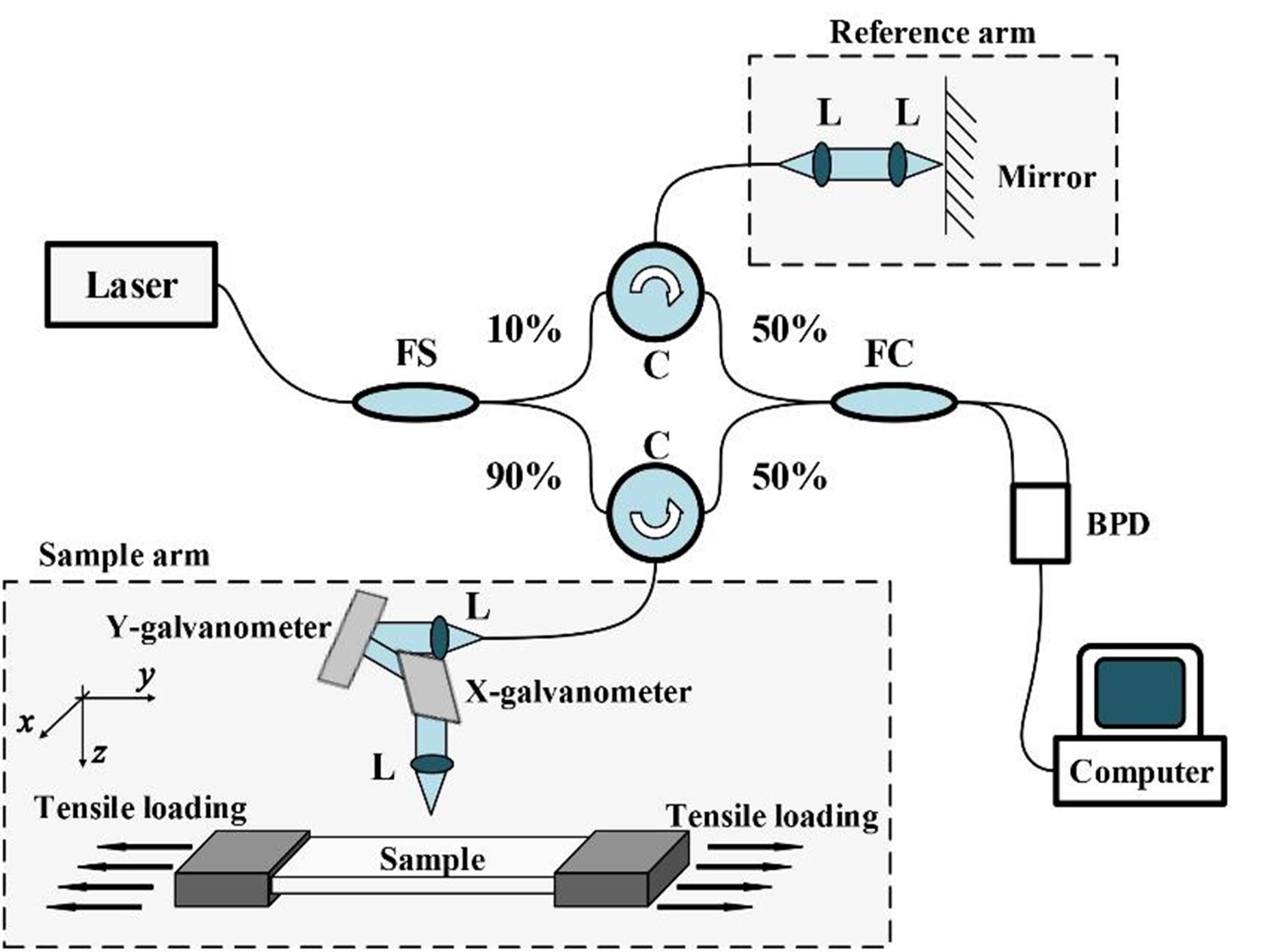
Figure 16. Schematic diagram of the OCE system, illustrating the optical path for detecting mechanically induced tissue deformation. FS, fiber splitter; FC, fiber coupler; BPD, balanced photodetector; L, lens; C, circulator. Adapted from Ref. [62]
3.1.3. Intelligent Analysis and Efficient Reconstruction
Automated and intelligent image analysis is the key for OCT technology to achieve large-scale screening and objective quantification. Accurate segmentation of retinal layers is the basis for quantitative diagnosis of glaucoma, macular diseases and other conditions, and U-Net and a series of its performance-enhanced variant networks have become the benchmark architecture for completing such semantic segmentation tasks, achieving extremely high segmentation accuracy on multiple public datasets (as shown in Figure 17)[65].
In terms of intelligent disease classification, models based on classic convolutional neural networks such as ResNet and VGG have achieved accuracy, sensitivity and specificity close to or even exceeding those of senior ophthalmologists in the differential diagnosis of various retinal diseases such as diabetic macular edema and age-related macular degeneration[18,66]. To improve the clinical acceptability and credibility of deep learning models, visualization techniques such as class activation mapping are integrated into the classification network to intuitively display the image areas on which the model makes decisions, enhancing its "interpretability"[18].
However, the healthy development of this field faces severe data-related challenges. Important studies have clearly pointed out that when dividing the dataset, if it is not strictly ensured that all images from the same subject only appear in either the training set or the test set, it will lead to serious "data leakage", which makes the generalization performance of the model seriously overestimated, which sounds an alarm for the objective evaluation of algorithms[67-69].
In telemedicine, mobile healthcare or resource-constrained embedded and IoT device applications, the massive OCT three-dimensional data poses pressure on storage and transmission. Based on compressed sensing theory, combined with deep learning to design an end-to-end reconstruction network, high-quality image recovery can be achieved at a sampling rate far lower than the Nyquist sampling rate, significantly reducing the amount of original data (as shown in Figure 18)[70]. In addition, using generative adversarial networks for image super-resolution reconstruction or quality enhancement can also be regarded as an "intelligent compression" and reconstruction process to recover high-fidelity content from low-quality, low-information data[71]. Combining excellent transform domains such as dual-tree complex wavelet transform with dictionary learning also provides an effective way to obtain high-quality reconstruction under the compressed sensing framework (as shown in Figure 19)[72].
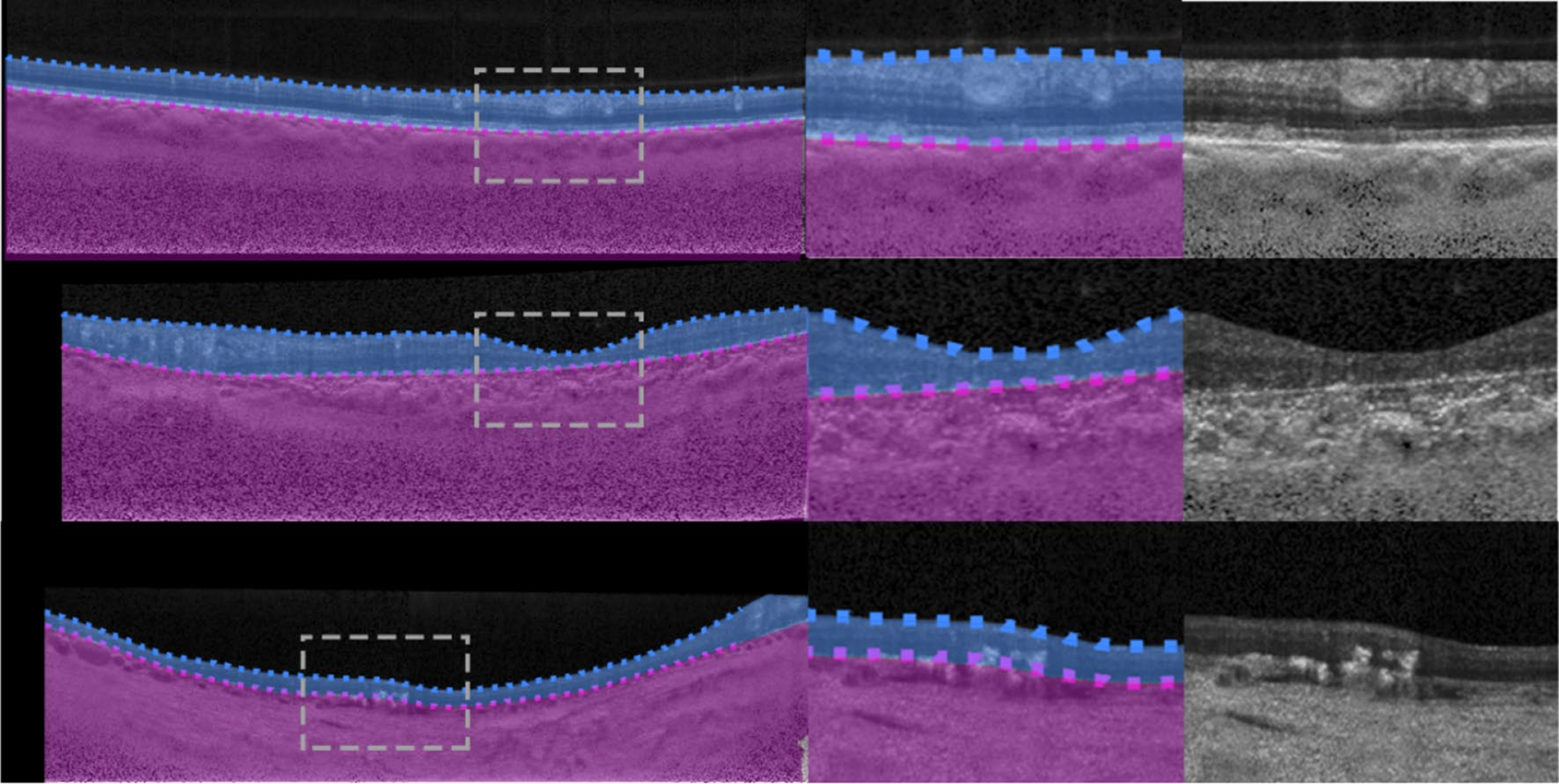
Figure 17. Example segmentation outputs from the R2 U-Net three-layer variant for the Stargardt disease dataset overlaid on OCT images. The full image and zoomed region show retina and choroid/sclera segmentation boundaries for quantitative layer analysis. Adapted from Ref. [65]
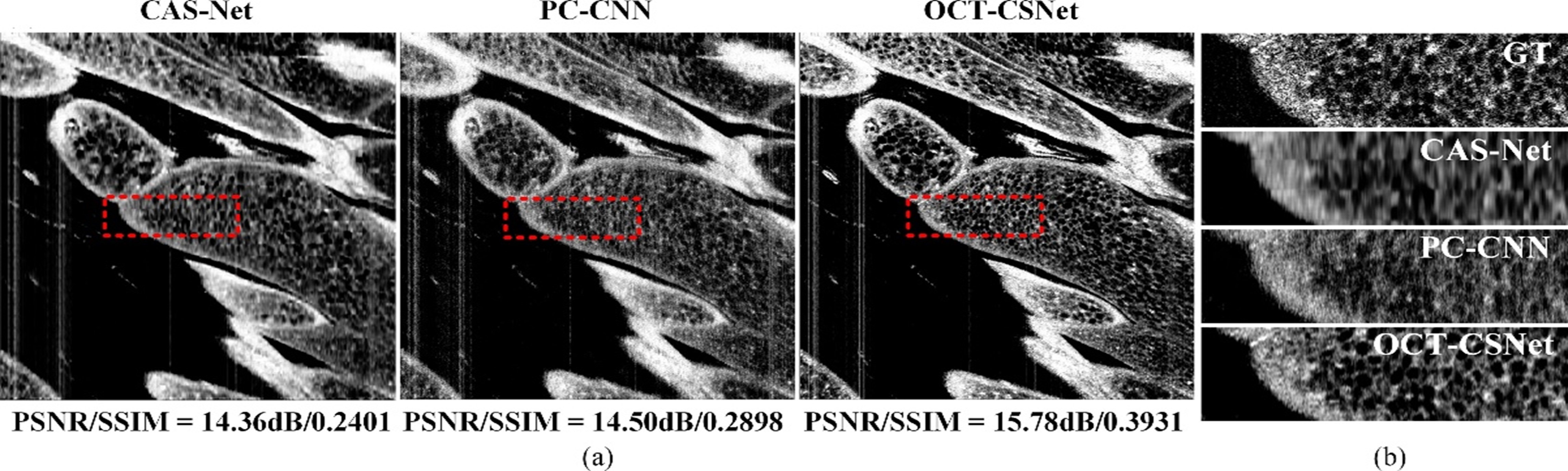
Figure 18. Comparison of compressed-sensing-based OCT reconstruction methods on en face views at a CS ratio of 0.01. (a) Overall reconstruction results. (b) Local magnification results, illustrating reconstruction fidelity under sparse sampling. Adapted from Ref. [70]
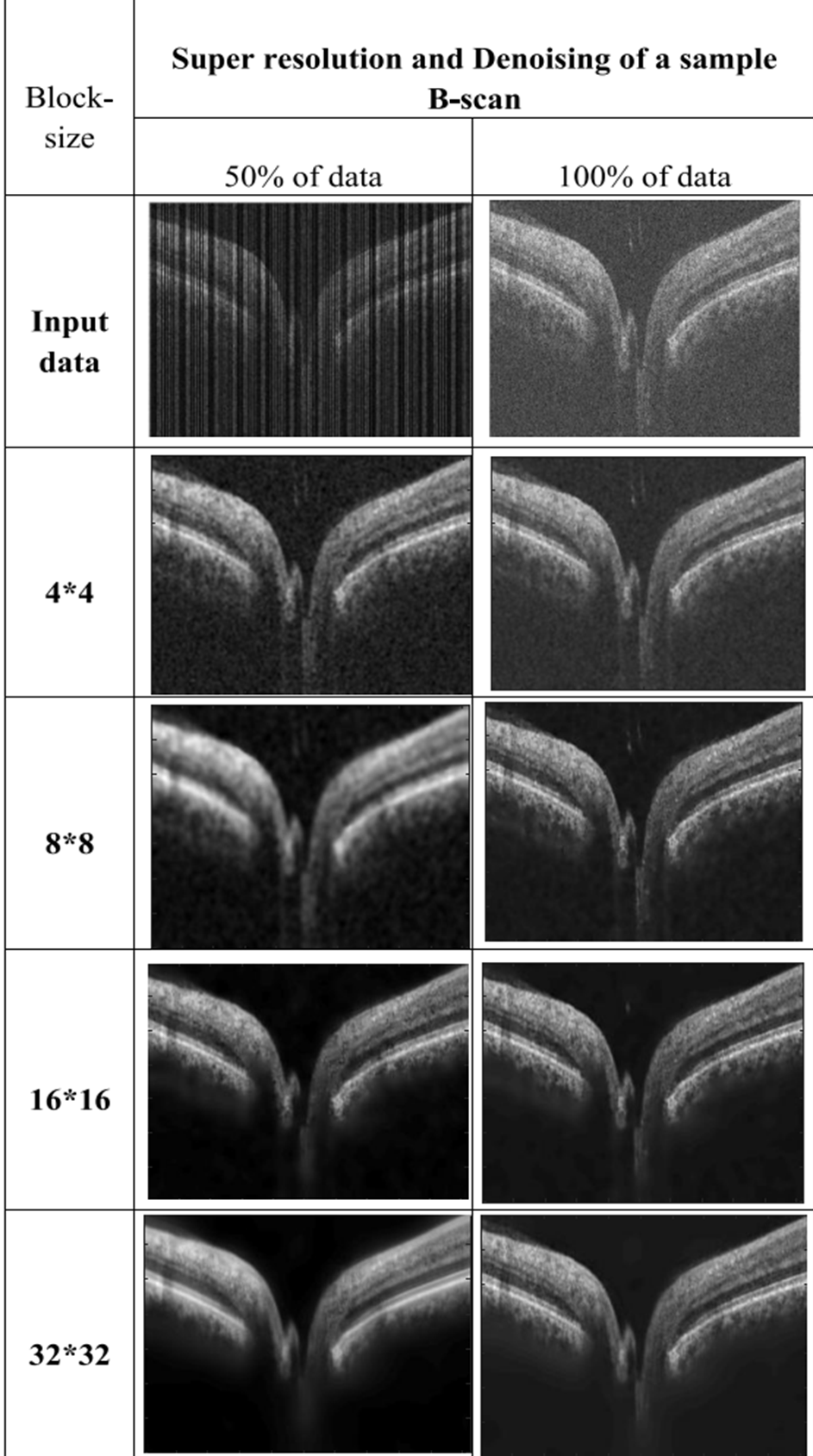
Figure 19. Comparison of reconstructed images based on complex wavelet transform, illustrating the effect of transform-domain sparse reconstruction on OCT image quality. Adapted from Ref. [72]
3.2. Core Bottlenecks and Future Breakthrough Paths of OCT Image Processing
Although existing OCT image processing algorithms have achieved the paradigm shift from model-driven to data-driven through deep learning, and have made leapfrog development in speckle noise suppression, image super-resolution enhancement, functional information extraction, and intelligent disease diagnosis, there are still four core bottlenecks restricting their clinical translation and large-scale application:
First, the algorithm model is disconnected from the OCT physical priors. Most existing algorithms directly apply general computer vision architectures without embedding the imaging physical laws such as the multiplicative coherent characteristics of speckle noise and the point spread function, resulting in the inability to fundamentally balance the contradiction between noise suppression and fine structure retention.
Second, the algorithm optimization objectives are mismatched with clinical diagnosis needs. Most algorithms take general indicators such as peak signal-to-noise ratio, structural similarity, and classification accuracy as optimization objectives, and are not deeply bound to the gold standard of clinical diagnosis. Denoising may change the characteristics of lesions and interfere with doctors' judgment, and classification models cannot provide diagnostic basis in line with clinical specifications.
Third, the generalization ability of the model is seriously insufficient and the cost of data annotation is high. The algorithm performance is highly dependent on single-center, single-device datasets, with a serious "domain shift" problem. Rare disease samples form a "long-tailed distribution", while the cost of fine-grained annotation is extremely high, resulting in a sharp contradiction between annotation requirements and data acquisition.
Fourth, algorithm research is separated from hardware system design, resulting in seriously insufficient software-hardware collaboration. Algorithms try to make up for the inherent defects of hardware but cannot completely reverse them, and hardware design does not incorporate algorithm requirements, resulting in the inability to provide high-quality raw data for algorithms, forming a development dilemma of "separate hardware and algorithm".
In view of the above core bottlenecks, combined with the development trend of artificial intelligence and medical imaging technology, the essential breakthrough of OCT image processing algorithms can be achieved through four core paths in the future:
First, by embedding imaging physical priors to construct a physically interpretable algorithm model, we can construct a differentiable optical simulator with optical system parameters, realize end-to-end physical consistency constraints between network output and interference spectrum, and make the algorithm shift from "data black-box fitting" to "physically consistent and interpretable modeling".
Second, by anchoring clinical diagnosis needs to construct interpretable and regulable clinical-grade algorithms[73], we can embed clinical diagnostic guidelines and quantitative criteria for lesions into the model training and evaluation system, and combine large language models to realize the automatic generation from OCT image analysis to clinical diagnosis reports.
Third, by breaking through the data dependency bottleneck to construct a few-shot and high-generalization learning paradigm, we can learn general feature representations through self-supervised pre-training, use cross-individual meta-learning to improve the adaptability to rare diseases, enhance cross-domain generalization ability through federated learning, and realize the unification of multi-device image styles combined with domain adaptation[74].
Fourth, by realizing full-link software-hardware collaboration to construct an intelligent system with a closed loop of "imaging-analysis", we can incorporate algorithm requirements in the hardware design stage, and deeply embed algorithms into the hardware acquisition process at the same time, driving the hardware to realize adaptive scanning and parameter adjustment through real-time feedback, forming a two-way closed loop of "intelligent imaging driven by diagnosis needs" and "parameter optimization driven by imaging quality".
4. Summary and Outlook
4.1. In-depth Integration of the Technological Development Context
At the hardware level, OCT technology has completed a fundamental transformation from the time domain to the Fourier domain. Through the continuous iteration of light sources, spectrometers, scanning mechanisms and integrated architectures, it has achieved an order-of-magnitude improvement in core indicators such as imaging speed, resolution, imaging depth and sensitivity. It has developed from a laboratory prototype device to a high-end medical device routinely used in clinical practice, and its application boundary has expanded from ophthalmology to multiple clinical disciplines and industrial cross-cutting fields. However, existing technologies have always been unable to break the inherent physical contradiction between resolution and imaging depth under the classical optical framework, and at the same time face the core bottlenecks that high performance is difficult to balance with miniaturization, low cost and clinical adaptability, as well as new challenges such as motion compensation for dynamic imaging, energy efficiency and thermal safety.
At the algorithm level, OCT image processing technology has completed the paradigm shift from classical model-driven to deep learning data-driven. From the initial basic preprocessing such as image denoising and enhancement, it has developed into a full-chain technical system including functional information extraction, intelligent segmentation and diagnosis, and efficient reconstruction. It not only makes up for the inherent defects of the hardware system, but also greatly expands the functional boundary and application value of OCT technology. However, existing algorithms still face the core pain points of disconnection from physical priors, mismatch with clinical needs, insufficient generalization ability, and lack of software-hardware collaboration, making it difficult to translate excellent laboratory performance into stable clinical practical value.
The two core arguments proposed in this paper accurately anchor the two core contradictions in the development of OCT technology, and also point out the core direction of future technological breakthroughs: only by realizing the principled innovation of the hardware system and the clinical-oriented reform of the algorithm system, and promoting the deep collaboration between the two, can we achieve the essential leap of OCT technology from "performance indicator iteration" to "clinical value implementation".
4.2. Future Trends and Core Challenges
For the future, OCT technology will further evolve along the core direction of "principle innovation, scenario customization, intelligent integration, inclusive popularization". First, new physical principles and new photonic devices will promote revolutionary breakthroughs in core performance. Cutting-edge technologies such as metasurface optics, quantum light sources, and integrated photonics are expected to fundamentally break the inherent limitation between resolution and imaging depth under the classical optical framework. The chip-level integrated "on-chip OCT" system will achieve an order-of-magnitude reduction in equipment volume and cost, laying the foundation for the popularization of the technology. Second, scenario customization will become the core logic of OCT system design, getting rid of the traditional path of "indiscriminately pursuing the ultimate indicators". For the core needs of different scenarios such as ophthalmology, cardiovascular, digestive tract, primary healthcare, and industrial testing, the hardware architecture and algorithm system are customized to achieve precise matching between technical indicators and clinical needs. Third, artificial intelligence will realize the deep embedding of the whole OCT process, and its role extends from back-end image analysis to mid-end real-time image processing and front-end intelligent scanning control. Through the physically interpretable AI algorithm embedded with physical priors, a fully automated closed loop from image acquisition, quality optimization to intelligent diagnosis is constructed. In addition, multi-modal fusion will realize panoramic analysis of multi-dimensional physiological and pathological information. The deep integration of OCT with photoacoustic imaging, fluorescence imaging, ultrasound imaging, Raman spectroscopy and other technologies can simultaneously obtain multi-dimensional information such as structure, blood flow, oxygenation, metabolism, biomechanics, and molecular characteristics at the system and probe levels, providing an unprecedented panoramic perspective for early diagnosis and precise treatment of diseases. Finally, technical standardization and open science will promote the healthy development of the industry. Establish unified standards covering image quality standards, algorithm performance evaluation benchmarks, data formats and interfaces, build large-scale, multi-center, high-quality public datasets, and strengthen prospective multi-center clinical research, laying a solid foundation for the standardized clinical translation and large-scale popularization of OCT technology with high-level evidence-based medical evidence.
4.3. Conclusion
After more than 30 years of development, optical coherence tomography has become a core technology in the field of biomedical imaging and industrial non-destructive testing, showing strong interdisciplinary characteristics and application potential. At present, OCT technology is at a critical turning point from "laboratory performance iteration" to "clinical value implementation", and from "qualitative structural imaging" to "quantitative functional diagnosis". Focusing on the two core dimensions of system hardware construction and image processing algorithms, this paper sorts out the research progress of the technology, analyzes the unsolved core bottlenecks, and puts forward the future breakthrough paths. For the future, only by adhering to the original innovation of basic research, taking the unmet clinical and industrial needs as the guidance, promoting the deep collaboration of hardware and algorithms, and the interdisciplinary integration of multiple disciplines, can we fully release the potential of OCT technology and make it play a greater value in protecting human health, exploring the mysteries of life, and ensuring industrial quality.
Author Contributions
Z.Z. conceived the review framework and drafted the manuscript; H.M. and R.T.L. collected and organized the literature related to OCT system construction and hardware development; F.Q.L. and M.C.G. summarized and analyzed the research progress in OCT image processing algorithms; H.D.W. and Q.C.G. assisted in reference organization, figure preparation, and manuscript revision; D.C. supervised the overall writing process, provided guidance and funding support, and revised and finalized the manuscript. All authors have read and approved the final manuscript.
Conflicts of Interest
The authors declare that the research presented in this paper has no commercial, financial, or personal relationships that could influence the objectivity, fairness, or integrity of the study.
Funding
Shandong Provincial Natural Science Foundation (ZR2022QF083); Taishan Scholar Youth Expert Program (tsqn202306254); Talent Introduction Program of Qilu University of Technology (2023RCKY033); Jinan Higher Education Innovation Project (2023GXRC062): Optical Fiber Sensing Technology for Oil and Gas Well Monitoring (Project Funding: 300,000 RMB, Implementation Period: 2024-2026)
References
-
D. Huang, E. A. Swanson, C. P. Lin, J. S. Schuman, W. G. Stinson, W. Chang, M. R. Hee, T. Flotte, K. Gregory, C. A. Puliafito, J. G. Fujimoto, “Optical coherence tomography.” Science 1991, 5035, 254, 1178-1181.
-
W. R. Gao, M. H. Hu, X. C. Yang, P. Li, D. Liu, “Review of Optical Coherence Tomography.” Collected Works for the 90th Birthday of Mr. Wang Daheng & Proc. Acad. Conf. Chin. Opt. Soc. 2004, 983-989.
-
D. X. Lu, W. H. Fang, Y. Y. Li, J. H. Li, X. J. Wang, “Principle and research progress of optical coherence tomography imaging technology.” Chin. Opt. 2020, 5, 13, 919-935.
-
Y. W. Qin, “Development, application and research status of optical coherence tomography imaging technology.” Laser J. 2015, 8, 36, 1-4.
-
Y. P. Chen, “Review on optical coherence tomography imaging.” Value Eng. 2014, 32, 33, 255-256.
-
R. Leitgeb, C. K. Hitzenberger, A. F. Fercher, “Performance of fourier domain vs. time domain optical coherence tomography.” Opt. Express 2003, 8, 11, 889-894.
-
M. A. Choma, M. V. Sarunic, C. Yang, J. A. Izatt, “Sensitivity advantage of swept source and Fourier domain optical coherence tomography.” Opt. Express 2003, 18, 11, 2183-2189.
-
M. Zeppieri, S. Marsili, E. S. Enaholo, A. O. Shuaibu, N. Uwagboe, C. Salati, “Optical coherence tomography (OCT): a brief look at the uses and technological evolution of ophthalmology.” Medicina 2023, 12, 59, 2114.
-
G. Xie, S. Wang, Y. Zhang, Y. Li, B. Hu, Y. Fu, Q. Yu, “Welding depth measurement for different mode lasers using optical coherence tomography.” Chin. Opt. Lett. 2024, 1, 22, 011203.
-
D. Wu, S. H. Gao, N. Zhang, Y. F. Lu, F. Xie, H. Zhang, S. Y. Ju, H. R. Zeng, C. M. Wang, “Research progress and application prospect of optical coherence tomography in forensic science.” Laser Optoelectron. Prog. 2023, 12, 60, 30-40.
-
M. F. Shirazi, R. E. Wijesinghe, N. K. Ravichandran, P. Kim, M. Jeon, J. Kim, “Quality assessment of the optical thin films using line field spectral domain optical coherence tomography.” Opt. Lasers Eng. 2018, 110, 47-53.
-
T. Tang, “Development and Application Research of Ultra-high Resolution Spectral-domain OCT System.” Dissertation, Zhejiang University, Hangzhou, 2017.
-
L. Milanovic, S. Milenkovic, N. Petrovic, N. Grujovic, V. Slavkovic, F. Zivic, “Optical coherence tomography (OCT) imaging technology.” IEEE 21st Int. Conf. Bioinform. Bioeng. 2021, 1-5.
-
Y. H. Xu, C. Qiu, Y. Y. Chen, Y. Wang, L. Liang, P. Jia, L. Qin, Y. Q. Ning, L. J. Wang, “Research progress of fast wide-tunable swept light sources for OCT applications.” Laser Optoelectron. Prog. 2023, 16, 60, 34-56.
-
S. Kim, M. Crose, W. J. Eldridge, B. Cox, W. J. Brown, A. Wax, “Design and implementation of a low-cost, portable OCT system.” Biomed. Opt. Express 2018, 3, 9, 1232-1243.
-
F. Li, Q. Wu, B. Jia, Z. Yang, “Speckle Noise Removal in OCT Images via Wavelet Transform and DnCNN.” Appl. Sci. 2025, 12, 15, 6557.
-
G. Chen, W. Wang, Y. Li, “Complex Correlated Phase Gradient Variance Based Optical Coherence Tomography Angiography.” IEEE Photonics J. 2023, 1, 15, 1-9.
-
O. Perdomo, H. Rios, F. J. Rodríguez, S. Otálora, F. Meriaudeau, H. Müller, F. A. González, “Classification of diabetes-related retinal diseases using a deep learning approach in optical coherence tomography.” Comput. Methods Programs Biomed. 2019, 178, 181-189.
-
H. Zhang, B. Yang, S. Li, X. Zhang, X. Li, T. Liu, R. Higashita, J. Liu, “Retinal OCT image segmentation with deep learning: A review of advances, datasets, and evaluation metrics.” Comput. Med. Imaging Graph. 2025, 123, 102539.
-
Y. X. Li, Y. P. Huang, J. J. Xu, J. Qin, L. An, G. P. Lan, “Progress of linear wavenumber spectral-domain optical coherence tomography.” Laser Optoelectron. Prog. 2025, 8, 62, 45-56.
-
N. A. Nassif, B. Cense, B. H. Park, M. C. Pierce, S. H. Yun, B. E. Bouma, G. J. Tearney, T. C. Chen, J. F. de Boer, “In vivo high-resolution video-rate spectral-domain optical coherence tomography of the human retina and optic nerve.” Opt. Express 2004, 3, 12, 367-376.
-
V. J. Srinivasan, Y. Chen, J. S. Duker, J. G. Fujimoto, “In vivo functional imaging of intrinsic scattering changes in the human retina with high-speed ultrahigh resolution OCT.” Opt. Express 2009, 5, 17, 3861-3877.
-
L. An, P. Li, G. Lan, D. Malchow, R. K. Wang, “High-resolution 1050 nm spectral domain retinal optical coherence tomography at 120 kHz A-scan rate with 6.1 mm imaging depth.” Biomed. Opt. Express 2013, 2, 4, 245-259.
-
B. K. Lee, S. Chen, E. M. Moult, Y. Yu, A. Y. Alibhai, N. Mehta, C. R. Baumal, N. K. Waheed, J. G. Fujimoto, “High-speed, ultrahigh-resolution spectral-domain OCT with extended imaging range using reference arm length matching.” Transl. Vis. Sci. Technol. 2020, 7, 9, 12.
-
M. H. Vafaie, M. Ansarian, H. Rabbani, “Design and Simulation of an Ultrahigh-resolution Spectral-domain Optical Coherence Tomography.” J. Med. Signals Sens. 2025, 4, 15, 12.
-
S. Chen, B. Potsaid, Y. Li, J. Lin, Y. Hwang, E. M. Moult, J. Zhang, D. Huang, J. G. Fujimoto, “High speed, long range, deep penetration swept source OCT for structural and angiographic imaging of the anterior eye.” Sci. Rep. 2022, 1, 12, 992.
-
S. Shin, U. Sharma, H. Tu, W. Jung, S. A. Boppart, “Characterization and analysis of relative intensity noise in broadband optical sources for optical coherence tomography.” IEEE Photonics Technol. Lett. 2010, 14, 22, 1057-1059.
-
Y. Wang, S. Chen, K. Lin, X. Chen, Z. Xu, S. Lou, X. Ge, G. Ni, X. Yu, J. Mo, Q. Mu, L. Liu, “Multi-channel spectral-domain optical coherence tomography using single spectrometer.” Chin. Opt. Lett. 2023, 5, 21, 051102.
-
Y. H. Ren, “Research on Spectral-Domain Optical Coherence Tomography and Its Applications.” Dissertation, Beijing Institute of Technology, Beijing, 2015.
-
C. Wang, “Research on Method and System of Orthogonal Dispersion Fourier-Domain Optical Coherence Tomography Imaging.” Dissertation, Zhejiang University, Hangzhou, 2013.
-
T. Liu, T. Pan, P. Wang, S. Qin, H. Xie, “Scanning optimization of an electrothermally-actuated MEMS mirror for applications in optical coherence tomography endoscopy.” Sens. Actuators A Phys. 2022, 335, 113377.
-
S. D. Gilinsky, E. J. Miscles, J. Musgrave, J. Bartos, S. W. Huang, V. M. Bright, J. T. Gopinath, “Nonmechanical spectral-domain optical coherence tomography using an electrowetting prism.” IEEE Photonics Conf. 2024, 1-2.
-
M. Nakada, C. Chong, A. Morosawa, K. Isamoto, T. Suzuki, H. Fujita, H. Toshiyoshi, “Optical coherence tomography by all-optical MEMS fiber endoscope.” IEICE Electron. Express 2010, 6, 7, 428-433.
-
Z. Duan, K. Huang, Z. Luo, K. Ma, G. Wang, X. Hu, J. Zhang, X. Luo, Y. Huang, G. Liu, X. Ding, P. Xiao, J. Yuan, “Portable boom-type ultrahigh-resolution OCT with an integrated imaging probe for supine position retinal imaging.” Biomed. Opt. Express 2022, 6, 13, 3295-3310.
-
K. Alsnaie, “Common path optical coherence tomography with electronic feedback for improved sensitivity.” Opt. Appl. 2023, 3, 53, 495-504.
-
X. Liu, X. Li, D. H. Kim, I. Ilev, J. U. Kang, “Fiber-optic Fourier-domain common-path OCT.” Chin. Opt. Lett. 2008, 12, 6, 899-901.
-
J. Kanngiesser, M. Rahlves, B. Roth, “Double interferometer design for independent wavefront manipulation in spectral domain optical coherence tomography.” Sci. Rep. 2019, 1, 9, 14651.
-
W. Li, Z. Wang, “Breaking the diffraction limit using fluorescence quantum coherence.” Opt. Express 2022, 8, 30, 12684-12694.
-
R. Chen, Y. Wu, K. Zhang, C. Liu, W. Li, Y. Chen, B. Shen, Z. Chen, H. Feng, Z. Ge, Y. Zhou, Z. Tao, X. Zhang, W. Xu, Y. Wang, P. Cai, D. Pan, H. Shu, L. Zhou, C. Wang, X. Wang, “Integrated bionic LiDAR for adaptive 4D machine vision.” Nat. Commun. 2026, 17, 24.
-
Y. Zhu, “Research on System Control and Image Processing of Optical Coherence Tomography.” Dissertation, Jinan University, Jinan, 2007.
-
H. T. Zeng, “Research on Speckle Noise Processing Methods of OCT Image Signals.” Dissertation, Chongqing University of Technology, Chongqing, 2025.
-
J. Zou, “Research on Signal and Image Processing in Spectral-Domain Optical Coherence Tomography.” Dissertation, Nanjing University of Aeronautics and Astronautics, Nanjing, 2015.
-
P. S. Arun, V. P. Gopi, P. Palanisamy, “Despeckling of OCT images using DT-CWT based fusion technique.” Optik 2022, 263, 169332.
-
X. Zhang, Z. Li, N. Nan, X. Wang, “Denoising algorithm of OCT images via sparse representation based on noise estimation and global dictionary.” Opt. Express 2022, 4, 30, 5788-5802.
-
M. Geng, X. Meng, L. Zhu, Z. Jiang, M. Gao, Z. Huang, B. Qiu, Y. Hu, Y. Zhang, Q. Ren, Y. Lu, “Triplet cross-fusion learning for unpaired image denoising in optical coherence tomography.” IEEE Trans. Med. Imaging 2022, 11, 41, 3357-3372.
-
Y. Li, Y. Fan, H. Liao, “Self-supervised speckle noise reduction of optical coherence tomography without clean data.” Biomed. Opt. Express 2022, 12, 13, 6357-6372.
-
C. Ge, X. Yu, M. Li, J. Mo, “OCT Speckle noise reduction based on a self-supervised B2U Network.” IEEE 10th Int. Conf. Inf. Commun. Netw. 2022, 489-494.
-
S. Li, M. A. Azam, A. Gunalan, L. S. Mattos, “One-step enhancer: Deblurring and denoising of OCT images.” Appl. Sci. 2022, 19, 12, 10092.
-
B. Yang, Y. Huang, Y. Xie, J. Li, S. Jia, Q. Hao, “Time-step encoded high-frequency enhanced diffusion model for OCT retinal image denoising.” Biomed. Opt. Express 2025, 11, 16, 4571-4587.
-
H. M. Salinas, D. C. Fernández, “Comparison of PDE-based nonlinear diffusion approaches for image enhancement and denoising in optical coherence tomography.” IEEE Trans. Med. Imaging 2007, 6, 26, 761-771.
-
L. Fang, S. Li, R. P. McNabb, Q. Nie, A. N. Kuo, C. A. Toth, J. A. Izatt, S. Farsiu, “Fast acquisition and reconstruction of optical coherence tomography images via sparse representation.” IEEE Trans. Med. Imaging 2013, 11, 32, 2034-2049.
-
G. Gong, H. Zhang, M. Yao, “Speckle noise reduction algorithm with total variation regularization in optical coherence tomography.” Opt. Express 2015, 19, 23, 24699-24712.
-
L. Fang, S. Li, D. Cunefare, S. Farsiu, “Segmentation based sparse reconstruction of optical coherence tomography images.” IEEE Trans. Med. Imaging 2016, 2, 36, 407-421.
-
R. Li, H. Yin, J. Hong, C. Wang, B. He, Z. Chen, Q. Li, P. Xue, X. Zhang, “Speckle reducing OCT using optical chopper.” Opt. Express 2020, 3, 28, 4021-4031.
-
N. You, L. Han, D. Zhu, W. Song, “Research on image denoising in edge detection based on wavelet transform.” Appl. Sci. 2023, 3, 13, 1837.
-
C. H. Liu, Y. W. Lee, Y. S. Chen, Y. C. Chen, S. L. Huang, “Deep Generative Network for Cellular-Resolution Optical Coherence Tomography Image Denoising.” IEEE J. Sel. Top. Quantum Electron. 2025, 4, 32, 1-11.
-
Z. Yuan, D. Yang, Z. Yang, J. Zhao, Y. Liang, “Digital refocusing based on deep learning in optical coherence tomography.” Biomed. Opt. Express 2022, 5, 13, 3005-3020.
-
N. Abbasi, K. Chen, A. Wong, K. Bizheva, “Computational approach for correcting defocus and suppressing speckle noise in line-field optical coherence tomography images.” Biomed. Opt. Express 2024, 9, 15, 5491-5504.
-
M. Lee, H. Bang, E. Lee, Y. Won, K. Kim, S. Park, H. Yoo, S. Lee, “Lateral image reconstruction of optical coherence tomography using one-dimensional deep deconvolution network.” Lasers Surg. Med. 2022, 6, 54, 895-906.
-
K. C. Zhou, R. P. McNabb, R. Qian, S. Degan, A.-H. Dhalla, S. Farsiu, J. A. Izatt, “Computational 3D microscopy with optical coherence refraction tomography.” Optica 2022, 6, 9, 593-601.
-
A. Javed, A. Khanna, E. Palmer, C. Wilde, A. Zaman, G. Orr, D. Kumudhan, A. Lakshmanan, G. D. Panos, “Optical coherence tomography angiography: a review of the current literature.” J. Int. Med. Res. 2023, 7, 51, 03000605231187933.
-
V. Y. Zaitsev, “Optical coherence tomography in elastography and angiography.” Usp. Fiz. Nauk 2023, 8, 193, 845-871.
-
H. Wu, J. Wang, Z. Zhu, H. Yu, H. Xie, R. Fang, Z. Li, “Impact of multiplicative noise removal on digital volume correlation-based optical coherence elastography.” Opt. Lasers Eng. 2025, 193, 109097.
-
X. Lin, J. Chen, Y. Hu, X. Feng, H. Wang, H. Liu, C. Sun, “Image quality assessment for digital volume correlation-based optical coherence elastography.” Photonics 2022, 8, 9, 573.
-
J. Kugelman, J. Allman, S. A. Read, S. J. Vincent, J. Tong, M. Kalloniatis, F. K. Chen, M. J. Collins, D. Alonso-Caneiro, “A comparison of deep learning U-Net architectures for posterior segment OCT retinal layer segmentation.” Sci. Rep. 2022, 1, 12, 14888.
-
K. Karthik, M. Mahadevappa, “Convolution neural networks for optical coherence tomography (OCT) image classification.” Biomed. Signal Process. Control 2023, 79, 104176.
-
I. E. Tampu, A. Eklund, N. Haj-Hosseini, “Inflation of test accuracy due to data leakage in deep learning-based classification of OCT images.” Sci. Data 2022, 1, 9, 580.
-
V. Koch, O. Holmberg, H. Spitzer, J. Schiefelbein, B. Asani, M. Hafner, F. J. Theis, “Noise transfer for unsupervised domain adaptation of retinal oct images.” Med. Image Comput. Comput. Assist. Interv. 2022, 699-708.
-
Y. Zhou, J. Li, M. Wang, Y. Peng, Z. Chen, C. Yao, T. Wang, L. Wang, W. Zhu, F. Shi, X. Chen, “DHNet: High‐resolution and hierarchical network for cross‐domain OCT speckle noise reduction.” Med. Phys. 2022, 9, 49, 5914-5928.
-
X. Guo, T. Zhang, K. Song, P. Wang, X. Han, M. Yu, X. Yi, X. He, T. Zhang, “Efficient OCT Image Reconstruction via Deep Compressed Sensing for Intelligent IoT Devices.” IEEE Internet Things J. 2025, 19, 12, 39890-39909.
-
T. T. Yu, D. Ma, J. Cole, M. J. Ju, M. F. Beg, M. V. Sarunic, “Spectral bandwidth recovery of optical coherence tomography images using deep learning.” 12th Int. Symp. Image Signal Process. Anal. 2021, 67-71.
-
M. Mokhtari, E. Yazdian, G. Plonka, H. Rabbani, “Application of Complex Wavelet Transform in OCT Image Compressive Sensing Reconstruction.” IEEE Access 2025, 13, 152934-152947.
-
Z. Yin, B. He, Y. Ying, S. Zhang, P. Yang, Z. Chen, Z. Hu, Y. Shi, R. Xue, C. Wang, S. Wang, G. Wang, P. Xue, “Fast and label-free 3D virtual H&E histology via active phase modulation-assisted dynamic full-field OCT.” npj Imaging 2025, 1, 3, 12.
-
S. Amgain, P. Shrestha, S. Bano, I. del Valle Torres, M. Cunniffe, V. Hernandez, P. Beales, B. Bhattarai, “Investigation of federated learning algorithms for retinal optical coherence tomography image classification with statistical heterogeneity.” arXiv 2024, arXiv:2402.10035.